
Resource Library
Your private library of tools, trackers, and protocols.
Next Q&A
Every 3rd Thursday of the month, Dr. Petteruti goes live on zoom at 10:00 AM (EST) for an open conversation about prostate health.
Link to the Call00
DAYS
00
HOURS
00
MINS
00
SECS

Guiding People Towards Living The 120 Lifespan While Retaining Youth
Long-form discussions on prostate health, anti-aging, and longevity. Find the clarity and context you rarely get from traditional care settings.
Helping you make informed decisions that support longevity and quality of life.
Listen To The Podcast



Show Notes
Not everyone has the time to sit down and listen to the full episodes. That’s why we created detailed show notes for every conversation on Dr. Petteruti’s podcast.
Here, you’ll find full written transcripts, key highlights, clinical insights, sources, and the most important takeaways from each episode.
Modern Healthcare Was Built to Treat Disease, Not Prevent It. That Model is Failing
Host: Intellectual Medicine by Dr. Stephen Petteruti (Member Version)
Date: 04 February, 2025
Episode Summary
- “Making America healthy again” begins with personal responsibility, because a nation cannot be treated like a patient, and health improves only when individuals change their daily habits.
- Modern healthcare often reacts to disease instead of preventing it, with insurance and medical spending focused on procedures and prescriptions rather than exercise, nutrition, and foundational care that keep people well.
- Hormones, peptides, and other therapies can support vitality when used thoughtfully and monitored carefully, while rushed or profit-driven protocols often ignore individual needs and create unnecessary risk.
- Breakthrough drugs and aggressive cancer treatments are frequently marketed as major advances, yet real-world benefits may be small while costs, side effects, and disruptions to daily life remain significant, which calls for careful evaluation before agreeing to intervention.
- Long-term health depends on prevention, including lowering toxin exposure, questioning invasive procedures such as unnecessary biopsies, and taking steady control of lifestyle decisions that protect strength, energy, and independence over time.
Quick Decision Checklist
Use this checklist as a simple self-review. These points help you confirm that your daily choices support prevention, personal responsibility, and long-term vitality rather than relying only on treatment after problems appear.
☐ You set aside time and resources for prevention such as regular movement, balanced meals, quality sleep, and routine health monitoring.
☐ Your daily habits support steady energy, healthy weight, and metabolic stability throughout the year.
☐ Your spending supports wellness through fitness, clean food, and foundational care alongside your insurance coverage.
☐ Your environment reflects lower exposure to avoidable risks such as smoking and unnecessary toxin contact.
☐ Your focus remains on consistent, everyday behaviors that protect strength, clarity, and independence over the long term.
00:00 Introduction
When you check the internet, you will see headlines like, “Only 12% of American adults are metabolically healthy.” After reading something like that, it is hard not to wonder where you stand. Are you actually healthy, or simply moving through life without obvious symptoms?
The idea of “making America healthy again” sounds straightforward, yet it raises a deeper question. When exactly were we healthy to begin with? Every period people look back on carried its own risks, from fatal infections before antibiotics, to pandemic disease, to waves of heart attacks and chronic illness. Health has never been a perfect state that disappeared. It has always required consistent effort and personal responsibility.
Waiting for a system, a policy, or the next medical breakthrough to fix things rarely leads anywhere. A country cannot be treated like a patient, and no one from outside is coming to manage your daily habits for you. Years of studying human behavior has showed us one thing: Real improvement begins at the individual level. The choices you make about how you eat, move, rest, and protect your body will eventually make a lot of differences.
02:52 The Reality of Health Insurance
Health insurance takes a significant share of personal income each year, and the national numbers show just how large that share has become. In 2024, U.S. healthcare spending grew 7.2% to $5.3 trillion, which averages $15,474 per person, with private insurance accounting for 31% of total expenditures. That amount of money represents a major financial commitment for families, employers, and the system as a whole.
With spending at that level, many people assume the structure is designed to keep them healthy, yet most coverage is centered on paying for care after illness has already developed. The system reimburses hospital visits, procedures, imaging, and medications, while the everyday habits that protect long-term health such as regular exercise, nutrition guidance, hormone support, and preventive programs usually come out of pocket. As a result, treatment is financially supported, while prevention often becomes a personal expense.
This arrangement quietly influences behavior. Once premiums, deductibles, and co-pays are paid each month, there is less room left to invest in proactive steps that build strength and resilience. Over time, it becomes normal to spend thousands managing disease and hesitate to spend a fraction of that on maintaining health. The focus shifts toward reacting to problems rather than reducing risk in advance.
Seeing the system this way brings the responsibility back to the individual. Insurance can help with unexpected events and major interventions, yet day-to-day vitality still depends on steady choices around movement, food, sleep, stress, and foundational care. Those small decisions, repeated consistently, have a greater impact on long-term outcomes than any policy document or insurance card.
03:22 Hormone Therapy
Hormones regulate how the body produces energy, builds muscle, maintains bone strength, stabilizes mood, and supports clear thinking, so changes in these levels show up in daily life in ways that are easy to notice. When testosterone, thyroid hormones, or other key signals decline, the effects often appear as fatigue, weight gain, reduced strength, slower recovery, and loss of focus. These symptoms are commonly dismissed as “just aging,” yet they reflect measurable physiologic changes rather than an unavoidable loss of health.
Clinical evidence shows that hormone levels influence long-term outcomes, which is why balance is important. Lowering hormone levels too far produced clear harm to brain health, which demonstrates that hormones affect far more than appearance or performance and play a direct role in how the brain and body function.
The same principle applies when levels are too low. If excessive suppression creates risk, maintaining healthy physiologic ranges helps protect strength, metabolism, and mental clarity. The focus remains on correcting deficiency rather than pushing levels beyond normal. Blood work, symptoms, and regular follow-up guide each adjustment so care reflects the individual instead of a preset protocol.
A steady and monitored approach treats hormone care as part of preventive medicine. Stable levels support muscle mass, protect bone density, maintain cardiovascular function, and preserve cognitive performance, all of which influence independence and quality of life over time. When these systems remain supported, daily movement feels easier, thinking stays sharper, and energy remains more consistent.
Viewed this way, hormone therapy becomes a practical tool for maintaining function year after year, with the goal of keeping the body operating efficiently and reducing the gradual decline that many people accept as normal.
05:40 Understand Peptides
Peptides are often presented as something new or experimental, yet the term simply describes short chains of amino acids that act as signaling molecules inside the body. In practical terms, they are small proteins that help regulate communication between cells. Many familiar therapies already fall into this category. Insulin is a peptide. Several naturally occurring hormones are peptides. These compounds have been used in medicine for decades, which means the concept itself is not exotic or futuristic. It is basic biology.
Understanding this definition removes much of the mystery. A peptide is not automatically a miracle treatment or a shortcut to better health. It is simply a tool that influences a specific pathway. Each peptide has a different target and a different purpose. Some affect metabolism, some influence healing and inflammation, and others act on brain function or body composition. The effect depends on the molecule and the context, not the label.
This is why careful evaluation matters. A thoughtful approach starts with a clear clinical goal and works backward. The question is not whether someone wants peptides. The question is what problem needs to be addressed and what mechanism makes sense for that problem. Symptoms, lab results, and overall health status guide the decision. When care is individualized, treatment becomes deliberate and measured. When care is reduced to a preset package or a quick sale, outcomes become unpredictable.
Using peptides responsibly follows the same principles as any other therapy. The body is assessed first, the target is defined, and the response is monitored over time. This keeps the focus on physiology rather than marketing and keeps the patient from chasing trends that sound advanced but add little real value.
09:43 The Quicks and Mentality
Many people judge their health by looking around and comparing themselves to others their age. If everyone feels tired, gains weight, and slows down, those changes begin to look normal. Decline becomes something expected instead of something to question. This mindset creates a quiet form of resignation. When everyone around you is sinking at the same rate, the situation feels acceptable even though the overall direction is downward.
This way of thinking shows up clearly in lab interpretation. Results are often described as normal for a certain age group, which gives the impression that falling performance is natural and therefore harmless. A lower hormone level, weaker metabolism, or rising blood sugar may still fit inside a wide reference range, yet that does not mean the body is functioning well. It simply means many other people share the same decline.
Medicine provides many examples where accepting the average leads to missed opportunities. Studies of prostate cancer treatment show that aggressive intervention does not automatically improve survival. In the large STAMPEDE randomized trial, adding radiotherapy to the prostate in men with newly diagnosed metastatic disease did not improve overall survival for the full study population. More treatment did not translate into longer life. This finding reinforces a broader lesson: Doing something simply because it is customary does not guarantee benefit.
A proactive mindset looks different. Instead of asking whether a result is typical for an age group, the focus shifts to whether it supports strength, energy, and long-term function. Health is treated as something to maintain intentionally rather than something that fades with time. Small corrections made early often prevent larger problems later.
11:55 The ‘Breakthrough Drug’
The phrase breakthrough drug carries a strong emotional pull. It suggests a major advance and a clear improvement in outcomes. In practice, many new therapies offer modest gains that sound impressive in headlines yet look far less dramatic when the numbers are examined closely. A treatment may extend survival by only a few months, require intensive monitoring, and bring a high rate of side effects, yet still be marketed as a major step forward.
Looking at real outcome data helps put these claims in context. Cancer trials often measure survival in months rather than years, and adverse reactions are common. Radiation-based therapies, for example, carry documented risks that affect daily life. Reports of brachytherapy show persistent rectal and bowel complications in a meaningful percentage of patients, which can include bleeding, pain, and long-term functional issues. These effects illustrate a simple reality. Every intervention has a cost.
This does not mean treatment has no place. It means the benefit must clearly outweigh the burden. Extending life slightly while reducing quality of life through repeated hospital visits, isolation, or severe side effects is a tradeoff that deserves careful thought. Numbers such as survival time, complication rates, and financial cost should be examined plainly rather than wrapped in optimistic language.
A clear view of the data leads to steadier decisions. New does not automatically mean better and expensive does not mean effective. The goal remains practical and grounded, which is to protect function, preserve energy, and choose interventions that offer meaningful value rather than symbolic action.
16:52 Isolation After the Treatment
Some treatments are presented as precise and targeted, yet the practical consequences tell a different story. A therapy may be described as localized radiation or a focused intervention, but the precautions that follow often reveal that the effect is not limited to a small area. When patients are instructed to avoid close contact with family members, sleep separately, or isolate themselves for days after each dose, it becomes clear that the treatment reaches beyond the intended target.
These instructions carry weight because they change daily life in very real ways. Time that would normally be spent with a spouse or family is replaced with separation. Normal routines are interrupted. Weeks of recovery and restricted contact accumulate across multiple cycles. When this pattern repeats over several treatments, a large portion of the remaining time is spent managing side effects rather than living normally.
This practical burden deserves the same attention as the survival statistics. Extending life by a short interval has a different meaning when a significant share of that time involves isolation, hospital visits, and recovery. Quality of life becomes just as important as duration. A treatment plan should be evaluated not only by what it promises on paper, but by how a person will actually live during those months.
Looking at care this way encourages a steadier and more deliberate decision process. Instead of reacting to the word breakthrough or assuming that more treatment automatically equals better outcomes, the focus shifts to the full picture, which includes time, comfort, independence, and daily function. A choice that preserves connection and strength may carry more value than one that simply adds days under heavy medical supervision.
19:46 Cadmium Is Everywhere
Environmental exposure rarely receives the same attention as drugs or procedures, yet long-term contact with toxins can quietly shape health over decades. Cadmium is one of those exposures. It is a heavy metal found in soil, food, cigarette smoke, and industrial pollution, and small amounts accumulate gradually in the body over time. Because it builds up slowly, most people are unaware of how much they carry.
Research shows that this exposure is not trivial. A pooled analysis of multiple studies found that cadmium levels in prostate tissue and blood were significantly higher in men with prostate cancer than in healthy controls. This association does not depend on symptoms or headlines. It is measured directly in tissue and plasma. The closer the proximity to a known carcinogen, the greater the potential for cellular damage.
This finding supports a simple preventive principle. Reducing exposure and lowering body burden where possible is a practical step toward lowering long-term risk. Attention to food sources, smoking status, occupational contact, and detoxification strategies becomes part of routine health maintenance rather than an afterthought. Prevention often looks quiet and unremarkable, yet these small adjustments accumulate just as steadily as the exposure itself.
Focusing on environmental load also shifts the conversation away from waiting for disease to appear. Instead of reacting after a diagnosis, the goal becomes lowering risk factors before they create harm. This approach aligns with the broader theme of taking responsibility for what can be controlled today rather than relying solely on treatment tomorrow.
21:33 Never Biopsy a Prostate
A biopsy is often treated as a routine next step after an abnormal screening result, yet the procedure is still invasive and carries biological consequences. Passing a needle repeatedly through tissue disrupts the structure of the gland and creates a path through which cells can move. The act of sampling is not neutral. It alters the environment it is trying to measure.
Laboratory research has demonstrated that tumor cells can be displaced along the needle track during core needle biopsy. This mechanical spread has been documented in several cancers and supports the concern that puncturing a tumor may increase the chance of local dissemination. Even if the risk is small, it highlights that a biopsy is not simply a harmless diagnostic step.
At the same time, outcome data from prostate cancer management show that detecting and treating more disease does not always translate into longer life. Aggressive intervention often carries side effects such as incontinence, sexual dysfunction, and chronic discomfort, while survival differences remain limited in many early cases. When the benefit is uncertain and the harms are clear, the decision deserves careful thought.
Seeing these pieces together leads to a more cautious mindset. Information is valuable only when it changes management in a meaningful way. If the result will not alter the plan or improve outcomes, adding an invasive step may create more harm than clarity. A deliberate approach that weighs necessity, risk, and long-term impact helps protect both health and quality of life.
23:40 Trust Generic Drugs
Medication decisions are often shaped by marketing and headlines instead of long-term evidence. New drugs arrive with big promises and strong promotion, while older medicines continue to work quietly in everyday practice. A drug that has been used for many years carries something valuable, which is a long record of real-world results. Doctors understand how it behaves, what doses work, and what side effects to expect because millions of patients have already used it.
Generic drugs come from this history. They contain the same active ingredients and must meet the same safety and quality standards as brand-name versions, yet they cost less because the research and branding expenses have already been paid. That lower cost makes treatment easier to access and easier to sustain over time.
This trend will continue. Many high-cost brand-name drugs are losing patent protection between 2025 and 2033, which opens the door for more affordable and complex generic alternatives. As those patents expire, more treatments will move into the generic space, giving patients dependable options without the high price tag.
25:39 Take Control of Your Health
Daily health is shaped by consistent habits rather than occasional treatments. Steady decisions around food, movement, sleep, and medical care influence long-term outcomes far more than reacting after a problem appears. A practical plan begins with simple actions you can apply every day.
What to Do:
- Maintain a healthy body weight and waist size through regular physical activity and balanced meals built around whole foods, since stable body composition supports metabolism, hormone balance, and cardiovascular health.
- Check your labs at regular intervals and review trends over time so you understand how your body is changing and can address small shifts before they grow into larger issues.
- Correct hormone, thyroid, blood sugar, and nutrient imbalances early with proper evaluation and follow-up, because early adjustment helps preserve energy, strength, and mental clarity.
- Reduce exposure to environmental toxins by avoiding smoking, improving indoor air quality, and paying attention to food and water sources, since long-term accumulation of harmful substances increases disease risk.
- Ask clear questions before agreeing to procedures or medications and make sure each step has a meaningful benefit that justifies the cost and potential side effects.
- Use established treatments with long safety records, including generic medications when appropriate, so care remains predictable, affordable, and supported by years of real-world experience.
- Protect the basics each day by prioritizing consistent sleep, daily movement, and stress control, because these habits support nearly every system in the body and strengthen long-term resilience.
Taking these steps keeps control in your hands and builds health gradually through deliberate, informed action.
Key Takeaway
Health rarely improves through one dramatic change. It improves through steady, informed decisions repeated every day. Insurance, prescriptions, and procedures all have a role, yet they do not replace the basics that keep the body strong. Energy, strength, and long-term resilience come from maintaining healthy weight, balanced hormones, clean nutrition, regular movement, reduced toxin exposure, and thoughtful medical choices grounded in evidence.
The common thread across each topic in this episode remains simple and practical. Question interventions that add risk without clear benefit, rely on treatments with a long record of safety, pay attention to environmental exposures that accumulate quietly over time, and address small imbalances before they grow into larger problems. This approach shifts the focus away from reacting to disease and toward protecting function.
Call to Action
If you found this episode helpful, take a moment to rate and subscribe to the Intellectual Medicine podcast so you never miss future discussions grounded in evidence and practical decision-making. For a deeper look at the research, clinical reasoning, and preventive strategies behind this vitality-focused approach, you can explore Fight Cancer Like a Man, which walks through these concepts in clear, step-by-step detail you can apply to your own health. Member notes, clinical summaries, and extended guides are added regularly, so stay engaged and continue building your understanding with each new episode.
Join the Intellectual Medicine Community
- Membership (exclusive educational content and clinical resources): https://tinyurl.com/DrPetterutiMember
- Sign up for Dr. Steve’s Email Newsletter: https://www.drstephenpetteruti.com
- Learn more about Intellectual Medicine: https://www.intellectualmedicine.com
Connect with Dr. Petteruti
- LinkedIn: https://www.linkedin.com/in/drstephenpetteruti
- Instagram: https://www.instagram.com/dr.stephenpetteruti
- Facebook: https://www.facebook.com/dr.stephenpetteruti
Subscribe to the Intellectual Medicine Podcast
- Apple Podcasts: https://tinyurl.com/DrPetterutiApplePodcast
- Spotify: https://tinyurl.com/DrPetterutiSpotifyPodcast
Disclaimer
This podcast and accompanying materials are for educational purposes only and do not replace personalized medical care. The information presented is designed to support informed decision‑making and health literacy, not to diagnose or prescribe. Always consult your own qualified healthcare provider regarding personal health questions or treatment decisions.
© 2026 Stephen Petteruti, DO | All rights reserved. Reproduction or distribution without permission is prohibited.
References:
Hoffman, Karen E et al. “Patient-Reported Outcomes Through 5 Years for Active Surveillance, Surgery, Brachytherapy, or External Beam Radiation With or Without Androgen Deprivation Therapy for Localized Prostate Cancer.” JAMA vol. 323,2 (2020): 149-163. doi:10.1001/jama.2019.20675
Kishan, Amar U, and Patrick A Kupelian. “Late rectal toxicity after low-dose-rate brachytherapy: incidence, predictors, and management of side effects.” Brachytherapy vol. 14, 2 (2015): 148-59. doi:10.1016/j.brachy.2014.11.005
Ladjevardi, Sam et al. “Prostate biopsy sampling causes hematogenous dissemination of epithelial cellular material.” Disease Markers vol. 2014 (2014): 707529. doi:10.1155/2014/707529
Lane, Janet Athene et al. “Functional and quality of life outcomes of localised prostate cancer treatments (Prostate Testing for Cancer and Treatment [ProtecT] study).” BJU international vol. 130,3 (2022): 370-380. doi:10.1111/bju.15739
Parker, Christopher C et al. “Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): a randomised controlled phase 3 trial.” Lancet (London, England) vol. 392,10162 (2018): 2353-2366. doi:10.1016/S0140-6736(18)32486-3
Zhang, Liang et al. “Cadmium Levels in Tissue and Plasma as a Risk Factor for Prostate Carcinoma: a Meta-Analysis.” Biological trace element research vol. 172,1 (2016): 86-92. doi:10.1007/s12011-015-0576-0
Other Links:
The Real Obesity Problem: Aging Faster, Losing Muscle, and Getting It Wrong
Host: Intellectual Medicine by Dr. Stephen Petteruti (Member Version)
Date: 11 February, 2025
Episode Summary
- Human beings naturally carry higher body fat from birth, which means energy storage is built into normal biology, and controlling percent body fat requires structure rather than short-term dieting.
- Percent body fat and muscle mass provide a clearer measure of health than body weight alone, because excess fat increases metabolic and cardiovascular risk while preserved muscle supports strength, glucose control, and long-term function.
- Regular feeding times, adequate protein intake, and simple repeatable meals help regulate hunger hormones such as ghrelin, reduce overeating, and make daily intake predictable.
- Exercise improves strength, bone density, heart health, and mental well-being, yet fat loss depends primarily on consistent nutrition habits, with medication used only as supportive therapy when appropriate.
- Sustainable weight management comes from organized daily behaviors that can be repeated long term rather than temporary diets or extreme restrictions.
Quick Decision Checklist
Use this checklist to confirm that daily habits support healthy body composition and long-term health.
☐ Percent body fat or body composition tracked regularly
☐ Consistent feeding times maintained throughout the day
☐ Adequate protein included at each meal
☐ Fruit intake controlled and limited to structured meals
☐ Strength training performed weekly to protect muscle and bone
☐ Exercise used for fitness and conditioning rather than to offset excess intake
☐ Daily routine focused on prevention and long-term function
00:00 Introduction
Human beings are the fattest animals at the time of birth. There is no other organism on the planet that carries as much body fat when it enters the world. In most mammals, only about 2 to 3% of birth weight is fat, and chimpanzee newborns average about 3%. Humans begin life with substantially higher fat stores, which means energy conservation is part of normal human biology from day one.
A body designed to conserve energy does not lose fat easily. When energy intake exceeds energy use, the excess is stored as fat. Repeating that pattern day after day increases the percent body fat over time. That is just one of the many reasons why a lot of people are now dealing with obesity issues, even when they are putting in conventional efforts to lose weight.
Now the big question is: What can be done differently to get rid of obesity issues?
01:20 Two Main Things We Do
Human behavior follows two consistent drives. We seek pleasure, and we avoid pain. Nearly everything we do each day connects back to one of those two goals.
Eating fits directly into both.
Food removes the discomfort of hunger, which satisfies the drive to avoid pain, and at the same time, food activates reward pathways in the brain that release dopamine and other neurotransmitters, which creates a sense of pleasure. The brain quickly learns this connection, so eating becomes a behavior the body encourages again and again.
There is also a metabolic reason behind this pattern. The brain accounts for only about 2% of body weight, yet it uses close to 20% of the body’s daily energy. That high demand keeps appetite signals active throughout the day and explains why most people rarely feel “done” eating for long.
02:57 What Is a Calorie?
A calorie is a unit of energy used in thermodynamics. In scientific terms, one dietary calorie, which is technically a kilocalorie, represents the amount of energy required to raise one kilogram of water by one degree Celsius. The term helps researchers measure heat and energy output, yet it does not describe food in a practical or physical way.
People do not eat energy units. They eat portions of food. The stomach responds to the weight and volume of what is consumed, along with the balance of protein, fat, and carbohydrate. For that reason, translating every meal into numbers often creates a system that feels disconnected from normal eating behavior.
Long-term data reflect this problem. Large reviews that combine results from multiple diet trials report that calorie-restricted diets rarely lead to durable weight loss. Many participants regain lost weight within the first year, and most return to baseline within several years. The outcome appears repeatedly across different diet styles.
Managing intake through planned portions and structured meals fits daily life more naturally and allows eating habits to remain consistent over time, which supports better control of percent body fat.
04:32 What Happens With Diets
Dieting usually lowers body weight at first, yet the number on the scale does not tell you what was actually lost. Weight includes fat, muscle, water, and bone. When intake drops sharply, the body does not remove fat alone. It often breaks down muscle tissue and sheds water along with it.
Losing muscle creates a problem. Muscle drives daily energy use and supports metabolic rate. When muscle mass declines, the body burns fewer calories at rest, which makes future fat storage easier even if food intake stays the same. At that point, weight loss slows while fat regain becomes more likely.
Bone can also be affected. Rapid weight loss without adequate protein and resistance training has been associated with measurable reductions in bone density, particularly during aggressive restriction or drug-only approaches. Bone tissue does not rebuild quickly, which means that short-term weight loss can carry long-term consequences.
For this reason, focusing only on total weight can be misleading. Health improves when fat decreases and muscle is preserved. Any plan that reduces muscle or bone while lowering the scale moves the body in the wrong direction.
06:04 Cornerstone Elements
Once you understand how the body stores energy and how dieting affects muscle and metabolism, the next step becomes practical. Fat loss works better when eating follows structure instead of appetite.
Hunger is not a reliable guide. The body produces hunger signals throughout the day whether energy is needed or not, which means waiting until you feel hungry often leads to irregular eating and oversized portions. A more predictable approach comes from scheduling intake in advance.
This is where feeding times come in. A feeding time simply means a planned moment to fuel the body. It does not need to be a large sit-down meal. It can be small and simple, yet it occurs at a consistent time. Planning meals this way creates stable energy levels and reduces impulsive eating later in the day.
Protein becomes the foundation of each feeding time. The body relies on amino acids to maintain muscle tissue, produce hormones, and support basic metabolic functions. When protein intake is too low, the body breaks down muscle to supply those needs. Losing muscle lowers metabolic rate and makes fat control more difficult, which is why preserving muscle mass remains a priority during weight loss.
Consistency matters more than variety. Repeating similar foods and portions each day simplifies decisions and makes intake easier to control. When meals are predetermined, adherence improves and eating becomes a routine process rather than something driven by mood or convenience.
This structured approach turns fat loss into a controlled system. Scheduled feeding times, adequate protein, and predictable portions provide the foundation that supports healthier body composition over the long term.
10:08 The Perfect Body Fat
Body weight alone does not tell you whether someone is healthy. The number on a scale combines fat, muscle, water, and bone into one total, so it cannot show what actually improved or what declined. Two people can weigh the same and still have very different health profiles depending on how much of that weight comes from fat and how much comes from lean tissue.
Percent body fat gives a clearer picture. Excess body fat, especially around the abdomen, is associated with insulin resistance, cardiovascular disease, type 2 diabetes, joint degeneration, and shorter lifespan. Large population studies consistently report higher rates of metabolic disease as body fat rises, even when total weight falls within a “normal” range.
Clinical guidelines place healthy body fat ranges for men at roughly 10 to 20% and for women at roughly 18 to 28%, with some variation by age and activity level. Values that rise far above these ranges correlate with higher inflammation markers, poorer glucose control, and reduced physical performance.
Muscle tissue supports daily energy use, strength, and joint stability. When dieting leads to muscle loss, resting metabolic rate declines because the body burns fewer calories at rest. Lower energy use makes fat regain more likely. A program that reduces scale weight but reduces muscle can leave someone lighter while also weaker and less metabolically efficient.
Tracking body composition prevents this problem. Tools such as bioelectrical impedance analysis, DEXA scans, or skinfold measurements identify what is actually changing. Fat loss with preserved muscle indicates progress. Muscle loss signals the need for adjustment.
11:34 The Hormone Called Ghrelin
Hunger is controlled by hormones. One of the primary signals is ghrelin, which is produced in the stomach and communicates with the brain to stimulate appetite.
Ghrelin rises when the stomach is empty and falls after eating. This cycle repeats throughout the day and follows a predictable rhythm. Research also shows that ghrelin responds to timing. When meals occur at regular hours, the body prepares in advance and appetite remains moderate. When meals are skipped or delayed, ghrelin levels climb higher and hunger becomes intense, which often leads to overeating.
The speed of eating also influences intake. After food enters the stomach, it takes about 20 to 30 minutes for hormonal signals to reduce appetite. Eating too quickly during this period allows more food to be consumed before fullness registers.
Scheduled meals reduce these extremes. Regular feeding times limit long gaps, keep hunger signals controlled, and make portion sizes easier to manage. Consistency works with normal physiology rather than against it.
13:13 Food Variety Is Nonsense
The idea that every meal needs to be different sounds attractive, yet it often makes weight control harder. Constant variety increases decision-making and creates uncertainty about portion sizes and ingredients. Each new option introduces small changes that add up over time.
Repetition simplifies eating. Similar meals each day stabilize intake and remove unnecessary choices. Many structured nutrition programs use this approach. Athletes, military units, and clinical weight-management plans often rely on standardized menus because predictable meals produce predictable results.
Consistency also improves accuracy. Repeating portions makes it easier to understand how the body responds and allows small adjustments without recalculating everything. Protein intake, carbohydrate limits, and total food volume remain controlled with less effort.
This structure supports everyday eating while still allowing planned flexibility. Most body composition changes come from routine habits repeated across the week rather than occasional special events.
Taken together, monitoring body fat, managing hunger hormones, and using simple, repeatable meals create a practical system. The body responds well to predictable inputs, and that predictability makes fat loss easier to maintain over time.
16:22 Knowing Someone Is Healthy
Health cannot be judged by body size alone. A lower number on the scale does not automatically mean better health because weight includes fat, muscle, bone, and water all combined into one total. The scale cannot tell you what improved and what declined.
Objective measurements give clearer answers. Percent body fat, muscle mass, strength, blood pressure, fasting glucose, and cholesterol levels describe how well the body is actually working. These markers connect directly to disease risk and daily performance.
Muscle tissue plays a central role in this process. Muscle handles most of the glucose your body uses after meals and supports insulin sensitivity. More muscle improves blood sugar control and lowers the risk of metabolic disease. Bone density protects posture and reduces fracture risk as you age.
Body fat location also influences risk. Fat stored around the abdomen surrounds internal organs and releases inflammatory signals that contribute to heart disease and diabetes. Studies consistently link increasing waist size with higher cardiometabolic risk.
Health therefore comes down to function. Strength, energy, and stable lab values give a more reliable picture than appearance.
16:51 Hedonistic Eating
Food does more than provide fuel. It also connects people to family, culture, and celebration. Removing every enjoyable food often creates frustration and leads to overeating later.
Behavioral research supports this pattern. Strict restriction increases cravings and lowers long-term adherence. When people feel deprived, they tend to compensate with larger portions or unplanned snacks. That cycle disrupts progress.
Planning enjoyable foods works better. Choosing the time and portion ahead of time keeps intake controlled while still allowing enjoyment. A defined treat fits into the week without throwing off the entire routine.
This method replaces impulsive eating with deliberate eating. Impulsive choices happen when food appears suddenly and emotions guide the decision. Deliberate choices follow a plan. A plan creates consistency, and consistency keeps body fat under control.
18:50 The Real Benefits of Fruits
Fruit contains fiber, vitamins, minerals, and plant compounds that support overall health. These nutrients are valuable. Fruit also contains natural sugars, which add to total carbohydrate intake.
Carbohydrates influence insulin release. Frequent large spikes in insulin encourage the body to store energy as fat. This process does not change simply because the sugar comes from fruit.
Portion size determines the effect. A small serving of berries with a meal provides nutrients with modest carbohydrate intake. Multiple servings of high-sugar fruits throughout the day can equal the carbohydrate load of snack foods or desserts.
Clinical nutrition guidance often recommends limiting fruit to one serving at a time and pairing it with protein or fiber. This slows absorption and helps keep blood sugar steady.
Fruit supports health when used thoughtfully. Large or frequent portions add extra energy that the body stores.
20:43 The Role of Exercise
Exercise improves heart health, strength, balance, and mood. Regular activity lowers blood pressure, improves insulin sensitivity, and supports mental well-being. These benefits are well established.
Exercise alone does not remove large amounts of body fat. A typical 30-minute brisk walk burns about 150 to 200 calories, which can be replaced quickly with one snack or drink. The body also adapts by conserving energy later in the day, which reduces the total effect.
Most fat loss comes from controlling intake. Exercise protects muscle and improves health markers, but it does not offset excess eating.
Exercise should therefore support your structure rather than act as compensation for food.
What to Do
Use these habits to guide daily behavior:
- Schedule 3 to 5 feeding times and include protein at each meal.
- Measure percent body fat periodically instead of relying only on scale weight.
- Plan one or two controlled treats per week.
- Keep fruit portions small and pair them with protein or fiber.
- Perform strength training 2 to 3 times per week to protect muscle and bone.
- Use walking or light cardio for heart health, not to cancel out overeating.
- Keep meals simple and repeatable so intake stays predictable.
These steps create structure and make progress easier to maintain.
21:30 Pharmacology Influence
Obesity is recognized medically as a chronic metabolic condition. Some people benefit from medication support when lifestyle changes alone are not enough.
Certain medications reduce appetite or increase fullness. Older options such as phentermine have been used for decades and remain inexpensive. Newer GLP-1 medications, including semaglutide, slow stomach emptying and reduce hunger signals. Clinical trials report average weight reductions of about 10 to 15% over one year.
Medication still requires structure. Reduced appetite can lead to skipped meals and low protein intake, which increases the risk of muscle and bone loss. Studies have documented declines in lean mass when weight loss occurs without adequate nutrition.
Medication works best when combined with planned meals and strength training. Drugs assist the process. Daily habits determine the outcome.
Key Takeaway
Health is built through daily structure, not occasional effort. Percent body fat, muscle mass, and metabolic stability provide a clearer picture of wellness than body weight alone, which is why tracking body composition offers more useful guidance than watching the scale.
Planned meals, controlled portions, and consistent eating times help regulate hunger hormones and reduce overeating, while simple and repeatable food choices keep intake predictable. Enjoyable foods can still fit into the week when they are scheduled and limited rather than impulsive.
Exercise supports strength, bone health, and cardiovascular function, yet food intake remains the primary driver of fat loss. Medication can assist selected individuals, but it works best when paired with disciplined habits rather than used as a substitute for them.
Call to Action
For a broader explanation of the reasoning behind this perspective, Fight Cancer Like a Man by Dr. Stephen Petteruti presents these principles in a structured and practical format, outlining how to approach cancer prevention, screening, and treatment decisions with clarity.
Fight Cancer Like a Man by Dr. Petteruti: https://www.amazon.com/dp/B0GLZ9TL8N/
If you would like continued access to extended clinical notes and member-only discussions, you can join the Intellectual Medicine Community here:
- Membership: https://tinyurl.com/DrPetterutiMember
- Sign up for Dr. Steve’s email newsletter: https://www.drstephenpetteruti.com
- Learn more about Intellectual Medicine: https://www.intellectualmedicine.com
Connect with Dr. Petteruti:
- LinkedIn: https://www.linkedin.com/in/drstephenpetteruti
Instagram: https://www.instagram.com/dr.stephenpetteruti
Facebook: https://www.facebook.com/dr.stephenpetteruti
Subscribe to the Intellectual Medicine Podcast:
- Apple Podcasts: https://tinyurl.com/DrPetterutiApplePodcast
- Spotify: https://tinyurl.com/DrPetterutiSpotifyPodcast
To support deeper reflection, referenced studies explore the long-term outcomes of observation compared with intervention. These data examine survival, treatment-related complications, and the biological consequences of biopsy and hormone suppression. Reviewing this literature allows patients and clinicians to move beyond habit and consider a more individualized approach to prostate health.
Selected References
The following peer‑reviewed studies and reviews provide background evidence for the concepts discussed in Episode 02: “Obesity and Aging: The Secrets to Sustainable Weight Loss.” These references explore the biological role of body fat in humans from birth, the metabolic adaptations that promote fat preservation, and strategies that support healthy, sustainable fat loss through metabolism management rather than short‑term dieting. Together, they highlight how energy balance, muscle preservation, and hormonal regulation influence long‑term body composition and aging.
Brennan CS. Dietary fibre, glycaemic response, and diabetes. Mol Nutr Food Res. 2005;49(6):560‑570. doi:10.1002/mnfr.200500025
PubMed: https://pubmed.ncbi.nlm.nih.gov/15926172/
Center for Academic Research and Training in Anthropogeny (CARTA). Fatness at Birth. CARTA Website. https://carta.anthropogeny.org/moca/topics/fatness-birth. Accessed February 11, 2025.
Chen Y, Yang Y, Jiang H, Liang X, Wang Y, Lu W. Associations of BMI and Waist Circumference with All‑Cause Mortality: A 22‑Year Cohort Study. Obesity (Silver Spring). 2019;27(4):662‑669. doi:10.1002/oby.22423
PubMed: https://pubmed.ncbi.nlm.nih.gov/30807694/
Cummings DE, Purnell JQ, Frayo RS, Schmidova K, Wisse BE, Weigle DS. A preprandial rise in plasma ghrelin levels suggests a role in meal initiation in humans. Diabetes. 2001;50(8):1714‑1719. doi:10.2337/diabetes.50.8.1714
PubMed: https://pubmed.ncbi.nlm.nih.gov/11473029/
Fothergill E, Guo J, Howard L, et al. Persistent metabolic adaptation 6 years after "The Biggest Loser" competition. Obesity (Silver Spring). 2016;24(8):1612‑1619. doi:10.1002/oby.21538
PubMed: https://pubmed.ncbi.nlm.nih.gov/27136388/
Heymsfield SB, Wang Z, Baumgartner RN, Ross R. Human body composition: advances in models and methods. Annu Rev Nutr. 1997;17:527‑558. doi:10.1146/annurev.nutr.17.1.527
PubMed: https://pubmed.ncbi.nlm.nih.gov/9240939/
Kuzawa CW. Adipose tissue in human infancy and childhood: an evolutionary perspective. Am J Phys Anthropol. 1998;(Suppl 27):177‑209. doi:10.1002/(SICI)1096‑8644(1998)107:27+<177::AID‑AJPA7>3.0.CO;2‑B
PubMed: https://pubmed.ncbi.nlm.nih.gov/9881522/
Leidy HJ, Clifton PM, Astrup A, et al. The role of protein in weight loss and maintenance. Am J Clin Nutr. 2015;101(6 Suppl):1320S‑1329S. doi:10.3945/ajcn.114.084038
PubMed: https://pubmed.ncbi.nlm.nih.gov/25926512/
Leonard WR, Robertson ML, Snodgrass JJ, Kuzawa CW. Metabolic correlates of hominid brain evolution. Comp Biochem Physiol A Mol Integr Physiol. 2003;136(1):5‑15. doi:10.1016/S1095‑6433(03)00132‑6
PubMed: https://pubmed.ncbi.nlm.nih.gov/14527624/
Mann T, Tomiyama AJ, Westling E, Lew AM, Samuels B, Chatman J. Medicare's search for effective obesity treatments: diets are not the answer. Am Psychol. 2007;62(3):220‑233. doi:10.1037/0003‑066X.62.3.220
PubMed: https://pubmed.ncbi.nlm.nih.gov/17469900/
Phillips SM, Van Loon LJ. Dietary protein for athletes: from requirements to optimum adaptation. J Sports Sci. 2011;29 Suppl 1:S29‑S38. doi:10.1080/02640414.2011.619204
PubMed: https://pubmed.ncbi.nlm.nih.gov/22150425/
Raynor HA, Epstein LH. Dietary variety, energy regulation, and obesity. Psychol Bull. 2001;127(3):325‑341. doi:10.1037/0033‑2909.127.3.325
PubMed: https://pubmed.ncbi.nlm.nih.gov/11316011/
Srikanthan P, Karlamangla AS. Muscle mass index as a predictor of longevity in older adults. Am J Med. 2014;127(6):547‑553. doi:10.1016/j.amjmed.2014.02.007
PubMed: https://pubmed.ncbi.nlm.nih.gov/24561114/
Swift DL, Johannsen NM, Lavie CJ, Earnest CP, Church TS. The role of exercise and physical activity in weight loss and maintenance. Prog Cardiovasc Dis. 2014;56(4):441‑447. doi:10.1016/j.pcad.2013.09.012
PubMed: https://pubmed.ncbi.nlm.nih.gov/24438736/
Villareal DT, Chode S, Parimi N, et al. Weight loss, exercise, or both and physical function in obese older adults. N Engl J Med. 2011;364(13):1218‑1229. doi:10.1056/NEJMoa1008234
PubMed: https://pubmed.ncbi.nlm.nih.gov/21449785/
Wells JC. The evolution of human fatness and susceptibility to obesity: an ethological approach. Biol Rev Camb Philos Soc. 2006;81(2):183‑205. doi:10.1017/S1464793105006974
PubMed: https://pubmed.ncbi.nlm.nih.gov/16573852/
Wilding JPH, Batterham RL, Calanna S, et al. Once‑Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021;384(11):989‑1002. doi:10.1056/NEJMoa2032183
PubMed: https://pubmed.ncbi.nlm.nih.gov/33567185/
Wolfe RR. The underappreciated role of muscle in health and disease. Am J Clin Nutr. 2006;84(3):475‑482. doi:10.1093/ajcn/84.3.475
PubMed: https://pubmed.ncbi.nlm.nih.gov/16960159/
Disclaimer
This podcast and its accompanying materials are for educational purposes. They are intended to support thoughtful decision-making and improve health literacy. They are not a substitute for individualized medical advice, diagnosis, or treatment. Always consult your qualified healthcare professional regarding personal medical concerns.
© 2026 Stephen Petteruti, DO | All rights reserved. Reproduction or distribution without written permission is prohibited.
Why Early Treatment of Prostate Cancer May Be Ineffective: The Case for Conventional Therapies
Host: Intellectual Medicine by Dr. Stephen Petteruti (Members Version)
Date: 08 February, 2026
Episode Summary
- Early stage prostate cancer often progresses slowly, and long-term studies report little or no survival difference between immediate conventional treatment and careful observation, while surgery and radiation carry clear risks such as urinary leakage, erectile dysfunction, and bowel complications.
- PSA tests, biopsies, and imaging provide limited predictive certainty, and invasive procedures can introduce their own harms, so decisions work best when guided by trends, overall health, and thoughtful evaluation rather than reacting to a single result.
- A structured, prevention-focused approach that includes watchful waiting, immune support, lowering toxic exposures, and maintaining healthy body composition helps protect quality of life while allowing time to choose treatment only when it is truly necessary.
Quick Decision Checklist
Use this checklist to confirm that your daily choices support careful monitoring, prevention, and long-term prostate health.
☐ PSA levels tracked over time instead of reacting to one isolated result
☐ Abnormal PSA values repeated after rest and recovery to rule out temporary causes such as illness, stress, or recent activity
☐ Clear understanding of how a biopsy result would change management before agreeing to the procedure
☐ Regular follow-up visits are scheduled for monitoring rather than rushing into treatment
☐ Percent body fat and waist size are kept within healthy ranges to lower metabolic and cancer risk
☐ Sleep, nutrition, and physical activity are used daily to support immune function
☐ Environmental exposures, such as heavy metals or toxins evaluated when appropriate
☐ Decisions made calmly with complete information and personal values guiding the process
00:00 Introduction
A prostate cancer diagnosis can make anyone feel like they need to act fast. The word “cancer” carries weight, and the first instinct is often to remove it or treat it immediately before it spreads. Many people believe that earlier treatment always leads to better results.
Prostate cancer does not always behave that way. Research over many years has found that a large number of early prostate cancers grow slowly and stay inside the gland without causing symptoms or shortening life. At the same time, common treatments such as surgery and radiation can lead to urine leakage, sexual dysfunction, bowel problems, and other lasting complications. In some cases, the treatment creates more measurable harm than the cancer itself.
That creates an important question: If early treatment does not clearly improve survival, and the side effects can permanently change daily life, is rushing into surgery or radiation always the right move?
02:09 New Discoveries About Prostate Cancer
For many years, prostate cancer was treated with one basic idea in mind. If cancer is found early, remove it quickly. The assumption was that early surgery or radiation would naturally save lives.
Long-term research began to question that belief. As more men were followed over time, doctors noticed something unexpected. Many early prostate cancers grew very slowly and stayed confined to the prostate for years without causing symptoms. Some never affected lifespan at all. In other words, detection did not automatically mean danger.
Clinical trials helped clarify this pattern. One of the better-known examples is the PIVOT trial, where men with localized prostate cancer were split into two groups. One group had the prostate removed through surgery, and the other group received observation without immediate treatment. After more than a decade of follow-up, overall survival between the two groups looked nearly the same, and deaths specifically from prostate cancer were also similar. Removing the gland did not produce a clear survival advantage.
At the same time, the men who underwent surgery experienced higher rates of complications. Urinary leakage, erectile dysfunction, and surgical risks appeared more often in the treated group. These side effects affected daily life in ways that could not be reversed, while the expected survival benefit remained small or uncertain.
These findings changed how many specialists think about early disease. Prostate cancer often behaves differently from aggressive cancers such as pancreatic or lung cancer. Instead of spreading rapidly, it may remain slow and contained for long periods. Treating every early tumor as an emergency can lead to harm without a matching benefit.
This shift in understanding explains why some medical guidelines now accept observation, often called watchful waiting or active surveillance, as a reasonable first step for many men with early-stage prostate cancer. The goal becomes careful monitoring rather than immediate intervention, which allows treatment to be reserved for cases that show clear signs of progression.
When you look at the data this way, the decision starts to feel less urgent. Early detection still has value, yet immediate treatment does not always improve outcomes. Knowing that difference gives you room to think clearly and weigh the real risks and benefits before moving forward.
05:00 Potential Damage from Radiation
Radiation therapy is often presented as an option for men who want to avoid surgery. The idea sounds straightforward. The prostate remains in place, and the cancer is targeted and destroyed with focused radiation. Many people assume this approach avoids the risks that come with an operation.
Radiation still carries its own set of risks, and those risks can appear months or even years later. Radiation affects cancer cells and nearby healthy tissue because the prostate sits next to the bladder and the rectum. When those tissues absorb radiation, they can become inflamed or damaged over time.
Damage to the rectum is known as radiation proctitis. Men can develop chronic irritation, bleeding, pain, or difficulty controlling bowel movements. Damage to the bladder, called radiation cystitis, can lead to burning with urination, bleeding, or increased urgency and frequency. These problems may persist long after treatment ends and can interfere with daily comfort.
There is also a broader biological concern. Radiation itself is carcinogenic, which means it has the potential to damage DNA and increase the risk of future cancers. Studies that follow patients for many years have reported small but measurable increases in secondary malignancies after pelvic radiation, including bladder and blood-related cancers. The risk is not immediate, yet it exists because radiation works by injuring cells at a genetic level.
When the survival benefit is unclear or ambiguous, these trade-offs become important. Some treatments extend life, and people accept side effects as part of the cost. Long-term survival for early-stage prostate cancer often appears similar across different treatment paths, so side effects carry greater weight because they may reduce quality of life without adding measurable time.
Radiation can cause lasting bowel, bladder, and sexual problems. These complications may continue for years and can affect daily comfort and independence. At the same time, research has not established a clear survival benefit for early-stage prostate cancer. Many men at this stage feel completely well and have cancer that remains confined to the prostate. Starting radiation in that situation can introduce new health problems that did not previously exist, even though the person had no symptoms to begin with.
07:17 Prostate Cancer Found During Cadaveric Studies
Some of the clearest insights about prostate cancer came from autopsy research rather than hospital treatment rooms. Pathologists examined the prostate glands of men who died from unrelated causes such as heart disease, infections, or accidents. These men lived their entire lives without symptoms or treatment for prostate cancer, yet their tissues told a different story under the microscope.
When those glands were analyzed carefully, many contained small areas of prostate cancer that had never been detected while the men were alive. The tumors were often tiny, localized, and completely silent. They caused no pain, no urinary problems, and no limitation in daily life, which means the disease existed without creating noticeable harm.
The numbers reported in these studies are striking. Research has found incidental prostate cancer in roughly 20 to 30% of men over age fifty, and the rate increases steadily with age. In men in their seventies and eighties, more than half show microscopic cancer within the gland, and in very elderly groups the majority carry these small lesions.
These findings change how the disease should be interpreted. Prostate cancer appears to be common at the cellular level, especially as men grow older. Many tumors grow slowly and remain confined to the gland for years or decades without spreading or threatening life expectancy.
This helps explain the old medical saying that many men die with prostate cancer rather than from it. The presence of cancer cells alone does not guarantee danger, and detecting every small focus does not automatically improve survival. A diagnosis may create anxiety, yet the biological behavior of the tumor may remain quiet for a very long time.
This context becomes important when screening tests identify an elevated PSA or a small abnormality on imaging. The natural reaction is urgency, because the word “cancer” carries emotional weight. Autopsy data suggest that many early findings represent slow, contained disease that might never affect lifespan or function.
08:37 Cancer Patients Who Survived
Statistics and research papers help guide decisions, yet real clinical stories often make the point more clearly. Over the years, many men diagnosed with prostate cancer have chosen to avoid immediate surgery or radiation and have continued living full, active lives. These cases remind us that a diagnosis does not automatically equal rapid decline or shortened survival.
One example involved a man with a significantly elevated PSA who underwent a biopsy that confirmed prostate cancer. He declined surgery because he felt well and wanted to protect his daily function and independence. More than two decades later, he remained alive, active, and symptom-free, even though his PSA stayed high throughout that time.
Another case moved in the opposite direction. A man underwent early surgery to remove the prostate gland, and his PSA dropped to nearly zero after treatment. Despite that reassuring number, the cancer later spread to his spine and caused severe complications, which shows that a low PSA does not always guarantee protection from progression.
A third patient had biopsy-confirmed cancer and chose observation rather than immediate treatment. Years later, repeat testing showed no detectable cancer in the sampled tissue. This outcome highlights how some prostate lesions can remain quiet or even regress without aggressive intervention.
Stories like these do not replace research, yet they reflect what long-term studies also report. PSA values do not always predict behavior accurately, and early treatment does not always determine survival. The relationship between test results and real-world outcomes remains inconsistent, which makes automatic intervention difficult to justify.
These examples support a central idea that runs throughout this topic. Prostate cancer behaves differently from person to person, and many cases move slowly enough that immediate treatment does not change the long-term picture.
10:56 Biopsy Reliability and Risks
A biopsy sounds simple in theory. A small needle enters the prostate, collects tissue, and the lab checks for cancer cells. Many people assume the result gives a clear yes-or-no answer and makes the next step obvious. In practice, the process carries uncertainty, and that uncertainty affects both accuracy and safety.
The prostate is not sampled in its entirety during a biopsy. Multiple needles are inserted into different areas of the gland in a pattern that resembles random sampling. This method means some areas are tested while others remain untouched, so a small tumor can be missed, and a quiet or contained lesion can be detected even though it may never cause symptoms. The result depends heavily on where the needle happens to land.
Because of this sampling method, false negatives and false positives both occur. A negative result does not guarantee the absence of cancer, and a positive result does not automatically indicate a dangerous or fast-growing disease. Research has documented both underdiagnosis and overdiagnosis with prostate biopsies, which creates confusion and often leads to repeated procedures.
The procedure itself also carries physical risks. Passing needles through the rectal wall into the prostate introduces bacteria into deeper tissue, which can lead to infection. Some men develop fever, urinary retention, or bloodstream infections that require hospitalization and intravenous antibiotics. Bleeding in the urine, stool, or semen is also common for days or weeks after the procedure.
There is another concern that receives less attention. Inserting needles into a tumor disturbs the local environment of the gland. Some laboratory and surgical literature has documented the presence of cancer cells along needle tracks after biopsies in certain cancers, which raises questions about whether mechanical disruption can contribute to cell spread. The evidence does not provide absolute proof for prostate cancer, yet the possibility deserves careful thought before proceeding.
Decision-making becomes important at this point. A biopsy only makes sense when the result will change what you plan to do next. If a person has already decided against surgery or radiation, then confirming the presence of cancer may add anxiety without altering the treatment plan.
This is why many clinicians recommend stepping back before scheduling a biopsy. Clarifying your goals first helps determine whether the information will be useful or simply stressful. Testing should serve a clear purpose, and that purpose should align with how you intend to manage your health moving forward.
13:14 Consequences of Sticking Needles Inside
Placing a needle into any organ creates more than a simple sample. It disrupts tissue, causes local inflammation, and triggers a healing response. That reaction may be minor on the skin, yet it carries greater significance inside an organ that contains a known tumor. The prostate has a dense network of blood vessels and lymphatic channels, so any disturbance spreads fluid and cells through those pathways.
During a standard prostate biopsy, multiple cores are taken in one session. In many practices, 10 to 12 needle passes occur in different parts of the gland. Each pass creates a small channel that cuts through tissue and temporarily opens a pathway between the inside of the prostate and the surrounding circulation. From a mechanical standpoint, this process fragments tissue and releases cells into nearby spaces.
Cancer biology adds another layer to consider. Tumor cells already have the ability to detach and migrate. When tissue is punctured repeatedly, some cells can be dislodged from their original location. In other areas of medicine, pathologists have documented tumor cells deposited along needle tracks after biopsies of breast and liver lesions. This phenomenon is called needle-track seeding. It remains uncommon, yet it demonstrates that mechanical spread can occur under certain conditions.
Direct proof in prostate cancer remains limited, yet the concept remains biologically plausible. The prostate sits next to veins and lymphatic vessels that drain into the pelvis. Any disruption in that environment creates an opportunity for cellular movement. Even a small theoretical risk becomes relevant when the disease itself often grows slowly and may never threaten life.
The transcript emphasizes a practical question. If the next step after a positive biopsy involves surgery or radiation that may not improve survival, then the biopsy may introduce risk without offering clear benefit. Testing should help guide a decision. Testing that does not change management creates exposure without purpose.
There are also immediate complications to consider. Studies report infection rates of about 2 to 5% after transrectal prostate biopsy, with a smaller percentage requiring hospital care. Urinary retention, bleeding, and significant discomfort also occur. These events may sound rare on paper, yet they affect real people and can disrupt weeks of daily life.
The broader issue comes down to intent. When a test is ordered, it should answer a question that changes action. If the plan already involves monitoring and preserving quality of life, then repeated needle procedures may add stress and physical risk without moving care forward. Careful thought before intervention protects both the body and peace of mind.
15:44 PSA Monitoring and Its Limitations
PSA stands for prostate-specific antigen. It is a protein made by prostate cells and released into the bloodstream. The test measures how much of that protein is present in a small blood sample. On paper, it looks simple. A higher number appears to suggest a problem inside the gland.
In practice, PSA is a nonspecific signal. It rises for many different reasons that have nothing to do with dangerous cancer. Infection, inflammation, recent sexual activity, cycling, urinary retention, and even a routine digital exam can temporarily increase the value. Normal day-to-day biological variation also causes small fluctuations. A single elevated result often reflects irritation rather than disease.
Large screening studies help clarify this issue. When PSA testing became widespread, diagnosis rates increased sharply, yet mortality from prostate cancer changed only modestly. Many men were labeled with cancer that never progressed to symptoms. This pattern is called overdiagnosis. Autopsy studies support it, with microscopic prostate cancer found in a significant percentage of men who died from unrelated causes and never knew they had it.
The number itself also lacks a clear boundary. There is no natural line where PSA suddenly shifts from safe to dangerous. A value of 2, 4, or 6 does not automatically predict outcome. Some men with low PSA still harbor aggressive disease, while others live decades with high levels and no clinical impact. This overlap limits the test’s ability to guide life-changing decisions.
The typical response to a rising PSA often follows a predictable chain. The number increases, concern grows, and a biopsy is scheduled. That biopsy may lead to surgery or radiation. Each step introduces risk, yet the original signal may have been temporary or harmless. When the starting point is unreliable, every downstream step inherits that uncertainty.
Trend tracking sounds logical, yet it carries similar problems. Small changes over time may reflect laboratory variation or short-term inflammation. Treating every upward movement as an emergency can create repeated procedures without improving outcomes. Many clinicians now recommend repeating the test after several weeks under calm conditions before making any decision.
Monitoring still has a role. Used thoughtfully, PSA can provide background information while a person remains symptom-free. It works best as one piece of context rather than a trigger for immediate intervention. Numbers should inform reflection, not rush action.
17:22 The Watchful Waiting Process
Watchful waiting is a planned approach to care. It means treatment is not started immediately after a prostate cancer finding. Life continues as usual while the condition is monitored at regular intervals. Decisions are made gradually with new information gathered over time.
This approach was developed because early prostate cancer often progresses slowly. Many tumors remain confined to the gland for years without causing symptoms. Autopsy studies have identified small prostate cancers in a large number of older men who died from unrelated causes, which indicates that the disease can exist quietly without affecting lifespan. In these situations, the cancer was present but never became clinically important.
Clinical research reflects the same pattern. Long-term studies that compared immediate surgery with observation reported similar overall survival between the groups. The difference appeared in side effects. Men who underwent treatment experienced higher rates of urinary leakage, erectile dysfunction, and bowel complications. The men who were monitored avoided those complications while maintaining similar life expectancy.
Monitoring follows a clear structure. PSA levels are checked at scheduled times. Physical exams or imaging are performed when needed. Symptoms are reviewed during follow-up visits. Trends across months or years guide decisions rather than a single number or one test result. This method keeps care organized and reduces unnecessary procedures.
Quality of life remains a central part of the plan. Urinary control, sexual function, and daily comfort influence independence and well-being. Preserving these functions has practical value. Many men prefer to maintain normal activity while continuing observation and reserving intervention for situations where clear progression appears.
Time also supports better thinking. A cancer diagnosis can create fear and pressure to act quickly. A slower, structured process allows space to review evidence and consider personal priorities. Health decisions made with patience often align better with long-term goals.
20:01 Addressing Other Carcinogens
Cancer risk does not come from a single source. Cells change over time when they are exposed to repeated stress, inflammation, and toxic substances. Prostate tissue responds to the same biological forces that affect the rest of the body, which means overall health habits influence what happens inside the gland.
Environmental exposure plays a measurable role. Heavy metals such as cadmium, arsenic, and lead have been classified as carcinogenic in toxicology research. Cadmium receives special attention because it accumulates in the prostate and can remain in tissue for years. Occupational studies in industrial workers have linked higher cadmium exposure with increased rates of prostate cancer, which supports the idea that long-term buildup carries risk.
Testing for toxic burden provides useful information. Blood, urine, or provocative chelation testing can estimate how much of these metals are stored in the body. Identifying elevated levels gives you a clear target for intervention. Removing or lowering those exposures reduces one source of chronic cellular stress.
Body composition also fits into this picture. Excess body fat acts as active tissue that releases inflammatory chemicals and hormones. Higher inflammation creates an internal environment that favors cellular damage over time. Waist circumference and percent body fat correlate with higher rates of several cancers, including prostate cancer, which means fat reduction becomes part of prevention rather than appearance.
Nutrient status supports immune surveillance. The immune system identifies and removes abnormal cells every day. Vitamin D plays a role in immune regulation, and blood levels in the adequate range have been associated with improved immune function in many studies. Zinc concentrates heavily in prostate tissue and contributes to normal prostate biology, which explains why maintaining sufficient levels remains a common clinical recommendation.
These steps do not involve cutting or radiating tissue. They focus on strengthening the body’s natural defenses and lowering known stressors. Improving nutrition, reducing toxins, maintaining healthy body fat, and supporting immune function create conditions that favor stability inside the gland.
Addressing carcinogens becomes a practical prevention. Each small correction removes one burden from the system. Over time, those changes build a healthier internal environment that supports long-term function and lowers avoidable risk.
22:17 Pause and Contemplate
A prostate cancer diagnosis often triggers urgency. The phone rings, a number comes back high, or a biopsy report includes the word “cancer,” and the next thought quickly turns into action. Appointments get scheduled, procedures get discussed, and decisions start to feel rushed. Fear pushes the process forward faster than understanding.
Prostate cancer rarely behaves like an emergency. In many men, it grows slowly over years rather than weeks. That time window gives you space to think clearly, review the evidence, and decide what truly supports your long-term health. Slowing the process protects you from making permanent decisions based on temporary anxiety.
Deliberate thinking leads to better outcomes. When you step back and look at survival data, treatment risks, and your current quality of life, the picture becomes practical instead of emotional. The goal becomes preserving function and longevity together, not reacting to a single lab result.
What to Do
- Review your PSA trend over time instead of reacting to a single reading.
- Repeat abnormal tests when appropriate to rule out temporary causes such as infection, stress, or recent activity.
- Ask how any proposed procedure will change management before agreeing to it.
- Focus on daily health habits that support immune function, including sleep, nutrition, and regular movement.
- Measure and reduce excess body fat, since abdominal fat correlates with higher cancer and metabolic risk.
- Maintain adequate vitamin D and zinc levels as part of general immune support.
- Schedule follow-ups at planned intervals so monitoring remains organized rather than reactive.
These steps keep you involved in your care and give you control over what can be controlled today. Thoughtful action replaces panic, and steady, informed decisions protect both quality of life and long-term health.
Key Takeaway
Early-stage prostate cancer often grows slowly and may remain confined to the prostate for many years without affecting daily function or life expectancy. At the same time, surgery, radiation, biopsies, and hormone therapy carry well-documented risks that can permanently affect urinary control, sexual function, bowel comfort, muscle mass, and overall quality of life. When the survival benefit of immediate treatment remains uncertain, those risks deserve careful thought.
Clear decisions come from understanding the numbers and the biology, not from fear. Tracking PSA trends, reviewing imaging carefully, and addressing modifiable risk factors such as body fat, toxic exposures, sleep, and immune support gives you a practical way to protect your health while you evaluate your options. A measured, informed approach allows you to preserve function, maintain strength, and choose treatment only when it truly serves your long-term well-being.
Continue the Conversation
If this discussion raised new questions for you, there are related episodes that expand on these themes in greater detail:
EP10 – Managing an Elevated PSA: Avoiding Unnecessary Prostate Biopsies
E16 - Prostate Cancer Prevention Is Not About Fear | What Most Doctors Miss
For a broader explanation of the reasoning behind this perspective, Fight Cancer Like a Man by Dr. Stephen Petteruti presents these principles in a structured and practical format, outlining how to approach cancer prevention, screening, and treatment decisions with clarity.
Fight Cancer Like a Man by Dr. Petteruti: https://www.amazon.com/dp/B0GLZ9TL8N/
If you would like continued access to extended clinical notes and member-only discussions, you can join the Intellectual Medicine Community here:
- Membership: https://tinyurl.com/DrPetterutiMember
- Sign up for Dr. Steve’s email newsletter: https://www.drstephenpetteruti.com
- Learn more about Intellectual Medicine: https://www.intellectualmedicine.com
Connect with Dr. Petteruti:
- LinkedIn: https://www.linkedin.com/in/drstephenpetteruti
Instagram: https://www.instagram.com/dr.stephenpetteruti
Facebook: https://www.facebook.com/dr.stephenpetteruti
Subscribe to the Intellectual Medicine Podcast:
- Apple Podcasts: https://tinyurl.com/DrPetterutiApplePodcast
- Spotify: https://tinyurl.com/DrPetterutiSpotifyPodcast
To support deeper reflection, referenced studies explore the long-term outcomes of observation compared with intervention. These data examine survival, treatment-related complications, and the biological consequences of biopsy and hormone suppression. Reviewing this literature allows patients and clinicians to move beyond habit and consider a more individualized approach to prostate health.
Selected References
Wilt TJ, Jones KM, Barry MJ, et al. Follow‑up of prostatectomy versus observation for early prostate cancer. N Engl J Med. 2017;377(2):132‑142. doi:10.1056/NEJMoa1615869
Hamdy FC, Donovan JL, Lane JA, et al. 15‑year outcomes after monitoring, surgery, or radiotherapy for prostate cancer. N Engl J Med. 2023;388(10):798‑809. doi:10.1056/NEJMoa2214122
Donovan JL, Hamdy FC, Lane JA, et al. Patient‑reported outcomes after monitoring, surgery, or radiotherapy for prostate cancer. N Engl J Med. 2016;375(15):1425‑1437. doi:10.1056/NEJMoa1606221
Klotz L. Active surveillance for low‑risk prostate cancer. N Engl J Med. 2020;383:81‑82. doi:10.1056/NEJMe2011155
Schröder FH, Hugosson J, Roobol MJ, et al. Screening and prostate‑cancer mortality in a randomized European study. N Engl J Med. 2009;360(13):1320‑1328. doi:10.1056/NEJMoa0810084
Zelefsky MJ, Levin EJ, Hunt M, et al. Incidence of late rectal and urinary toxicity after conformal radiotherapy for prostate cancer: Dose‑response relationships. Int J Radiat Oncol Biol Phys. 2008;70(4):1124‑1129. doi:10.1016/j.ijrobp.2007.11.044
Sakr WA, Haas GP, Cassin BF, Pontes JE, Crissman JD. The frequency of carcinoma and intraepithelial neoplasia of the prostate in young male patients. J Urol. 1994;152(2 Pt 1):1011‑1014. doi:10.1016/S0022‑5347(17)32573‑4
Loeb S, Carter HB, Berndt SI, Ricker W, Schaeffer EM. Complications after prostate biopsy: data from SEER‑Medicare. J Urol. 2011;186(5):1830‑1834. doi:10.1016/j.juro.2011.07.005
Volanis D, Neal DE, Warren AY, Kelly JD. Incidence of needle‑tract seeding following prostate biopsy: a literature review. Urol Int. 2015;95(1):117‑121. doi:10.1159/000366175
Disclaimer
This podcast and its accompanying materials are for educational purposes. They are intended to support thoughtful decision-making and improve health literacy. They are not a substitute for individualized medical advice, diagnosis, or treatment. Always consult your qualified healthcare professional regarding personal medical concerns.
© 2026 Stephen Petteruti, DO | All rights reserved. Reproduction or distribution without written permission is prohibited.
Monthly Q&A
If you couldn't join the previous Q&As, you can watch the recordings here.
June 2026
May 2026
April 2026
March 2026
February 2026
January 2026
December 2025
November 2025
October 2025
Monthly Q&A
Every 3rd Thursday of the month, Dr. Stephen Petteruti goes live with the Men's Vitality Support Community for an open conversation about prostate health.
Watch the previous recordings here.
June 2026
May 2026
April 2026
March 2026
February 2026
January 2026
December 2025
November 2025
October 2025
Video Gallery
Find guides, intructions and the answer to your question, all in video format.
The Protocol
What you can eat and what you should avoid
Mistletoe Injection Training

Support Your Long-Term Health Through Smarter Nutrition
Find simple and practical meals, aligned with a prostate-conscious approach to inflammation, metabolic health, and hormone balance.
Optimizing your health doesn’t start with a prescription. t starts in the kitchen.
Baked Eggs in Avocado

Ingredients:
- 1 avocado
- 2 large eggs
- Salt and pepper
- Any herbs and hot sauce you like
Instructions:
- Cut an avocado in half and remove the pit.
- Scoop out a small portion of the flesh from each half to create a well for the eggs.
- Crack an egg into each avocado half, sprinkle with salt and pepper, and bake in the oven until the eggs are cooked to your liking.
- Serve with a sprinkle of herbs or a dash of hot sauce.
Serving size: one half avocado.
Makes 2 servings
Nutrition Information (per serving):
- Protein: 7g
- Carbohydrates: 9g
- Fat: 10g
- Fiber: 7g
Chocolate Hazelnut Waffles

Ingredients:
- 1 cup almond flour
- 2 tablespoons coconut flour
- 1/3 cup unsweetened cocoa powder
- 1/4 cup Swerve sweetener
- 2 teaspoons baking powder
- 1/4 teaspoon salt
- 1/3 cup hazelnut milk
- 3 eggs
- 2 tablespoons coconut oil, melted
- 1 teaspoon vanilla extract
- 1/3 cup chopped hazelnuts
- Sugar-free whipped cream (optional)
- Sugar-free chocolate chips (optional)
Instructions:
- Preheat your waffle iron.
- In a large mixing bowl, whisk together the almond flour, coconut flour, cocoa powder, Swerve sweetener, baking powder, and salt.
- In another mixing bowl, whisk together the hazelnut milk, eggs, melted coconut oil, and vanilla extract.
- Pour the wet ingredients into the dry ingredients and whisk until combined.
- Fold in the chopped hazelnuts.
- Grease the waffle iron with cooking spray or coconut oil.
- Scoop 1/4 cup of the batter onto the waffle iron and cook for 3-4 minutes, or until crispy on the outside and cooked through.
- Repeat until all the batter is used up.
- Serve the waffles with sugar-free whipped cream and sugar-free chocolate chips, if desired.
Makes 2 servings
Nutrition Facts (per serving):
- Protein: 10g
- Carbs: 9g
- Net Carbs: 4g
- Fat: 22g
- Fiber: 5g
Asian Glazed Meatballs with Zucchini Noodles

Ingredients:
For the meatballs:
- 1 lb. ground pork
- 1 egg
- 2 tbsp. coconut flour
- 2 cloves garlic, minced
- 1 tsp. ground ginger
- 1/2 tsp. sea salt
- 1/4 tsp. black pepper
- 1/4 cup chopped green onions (for garnish)
For the Asian Glaze:
- 2 tbsp. coconut aminos
- 1 tbsp. apple cider vinegar
- 1 tbsp. sesame oil
- 1 tbsp. minced fresh ginger
- 2 cloves garlic, minced
- 1/2 tsp. red pepper flakes
For the zucchini noodles:
- 3 large zucchini, spiralized
- 1 tbsp. coconut oil
- Salt and black pepper, to taste
- 1/4 cup chopped fresh cilantro (for garnish)
Instructions:
- Preheat oven to 375°F (190°C) and line a baking sheet with parchment paper.
- In a large mixing bowl, combine ground pork, egg, coconut flour, minced garlic, ground ginger, salt, and black pepper. Mix well until all the ingredients are well combined.
- Using a tablespoon, shape the pork mixture into small meatballs and place them on the prepared baking sheet.
- Bake for 15-20 minutes, or until the meatballs are fully cooked.
- While the meatballs are cooking, prepare the Asian glaze. In a small bowl, mix together the coconut aminos, apple cider vinegar, sesame oil, minced ginger, minced garlic, and red pepper flakes.
- In a separate skillet over medium heat, add the coconut oil and the zucchini noodles. Season with salt and black pepper and cook for 2-3 minutes, or until tender.
- Add the Asian glaze to the skillet with the cooked zucchini noodles and toss to coat evenly.
- Divide the zucchini noodles and meatballs evenly among four meal prep containers.
- Garnish with chopped green onions and fresh cilantro.
- Store in the refrigerator for up to four days.
Makes 4 servings
Nutrition Information (per serving):
- Protein: 25g
- Carbohydrates: 10g
- Fat: 35g
- Fiber: 3g
Note: This recipe can be adjusted to suit individual dietary needs or preferences. For example, if you need to increase your carb intake, you can serve the Asian glazed meatballs with a side of roasted sweet potatoes or brown rice, and if you need to reduce your fat intake, you can use lean ground pork or reduce the amount of sesame oil used in the recipe.
Baked Salmon and Roasted Asparagus

Ingredients:
- 4 salmon filets (4-6 oz each)
- 1 pound asparagus, tough ends trimmed
- 2 tablespoons olive oil
- 1 lemon, thinly sliced
- Salt and pepper, to taste
Instructions:
- Preheat the oven to 400°F.
- Place salmon filets on a baking sheet lined with parchment paper.
- Drizzle with olive oil and season with salt and pepper.
- Place lemon slices on top of the salmon.
- Bake for 12-15 minutes, or until the salmon is cooked through.
- While the salmon is cooking, toss the asparagus with olive oil, salt, and pepper in a separate baking dish.
- Place the asparagus in the oven with the salmon and roast for 10-12 minutes, or until the asparagus is tender.
- Serve the salmon and asparagus together.
Makes 4 servings
Nutrition information (per serving):
- Protein: 40g
- Carbs: 7g
- Net Carbs: 3g
- Fat: 25g
- Fiber: 4g
Downloadable Documents
Use these foundational guides and trackers to understand and organize your care protocol.
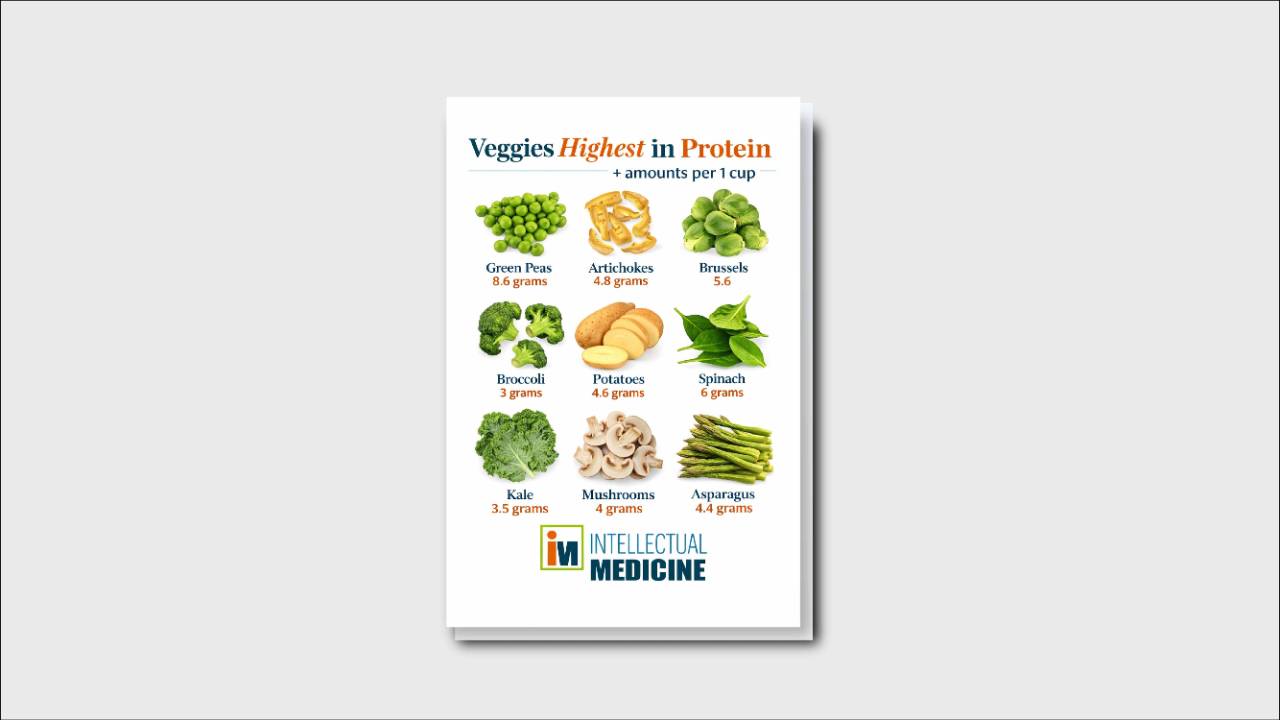
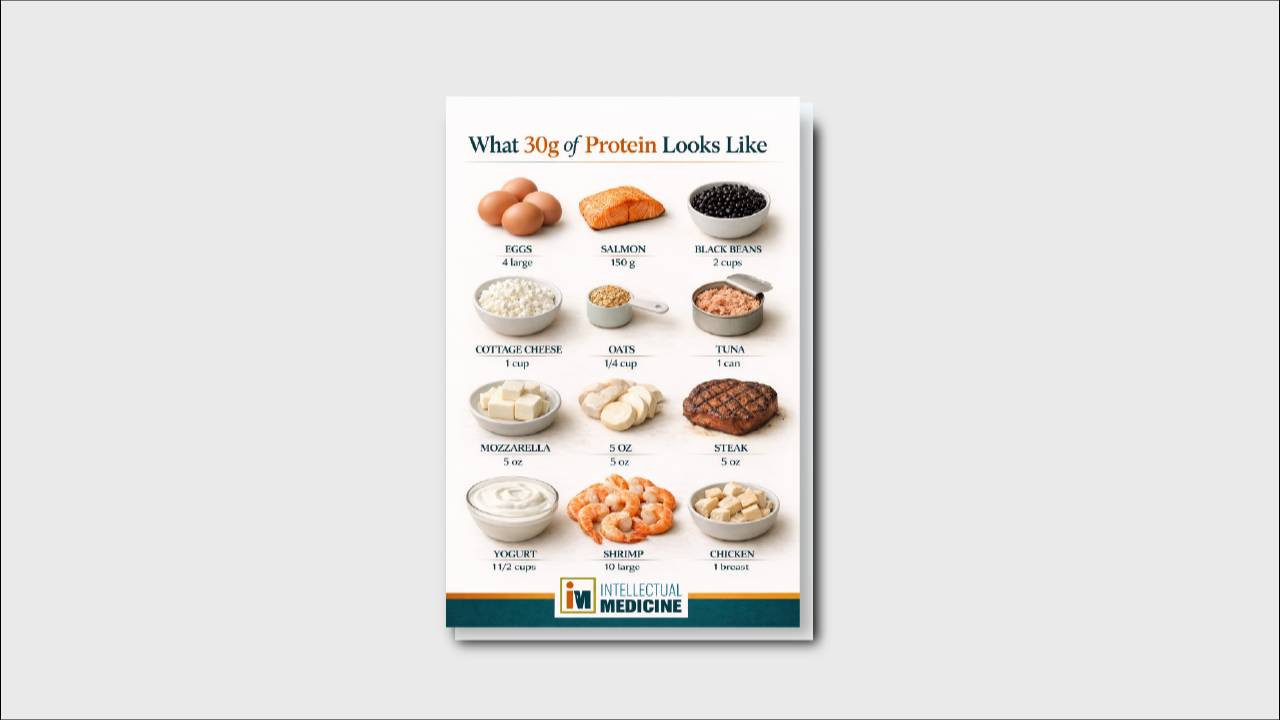
Research & Information
Does testosterone therapy help treat prostate cancer?
Treating men with testosterone does not increase the risk of developing prostate cancer. This fact is now well established and reverses decades of incorrect thinking regarding the association between testosterone and prostate cancer. In fact having a low testosterone level is a risk factor for developing prostate cancer.
Recent studies have demonstrated that the longer a man is on testosterone treatment, the lower his risk for developing prostate cancer.
A definitive study called the TRAVERSE trial was published in 2023. It observed men on testosterone therapy and were able to conclude that there is no increased risk of major cardiac event or strokes.
But how about for men who already have prostate cancer, or an elevated PSA with prostatic enlargement? Once again historical impressions have been proven incorrect. Testosterone therapy does not stimulate growth of the prostate gland. Therefore it is safe to use in men with symptomatic prostatic hypertrophy.
In addition there is a growing volume of studies demonstrating the safety of using prostate treatment in the setting of active prostate cancer. This raises a paradox. If prostate cancer is treated in some cases by lowering testosterone levels, how could it be that adding testosterone has therapeutic value?
The paradox can be explained by understanding how the prostate gland processes testosterone. The gland has a limited capacity for absorbing testosterone. This is referred to as the "testosterone saturation theory." The capacity for the prostate gland to absorb testosterone hormone appears to peak at 250 ng/dL blood level. This means that any testosterone above that threshold will have no bearing on the gland itself. PSA is a testosterone dependent protein. When a man with low testosterone begins testosterone therapy there is often an initial increase in PSA levels. This has nothing to do with cancer progression but is the result of testosterone stimulating more protein development. This process plateaus after about three months.
Imposing high testosterone on a prostate gland that is living in a low testosterone environment to can overwhelm the androgen receptors on the prostate cancer cells imposing harm. The sudden change in levels appears to disrupt the cancer cells DNA strands thus killing them. By cycling between high, and low levels of testosterone the possibility exists that a man can benefit from the vitality of testosterone while actually imposing harm on underlying prostate cancer cells.As always with prostate cancer, and for that matter life in general, your decisions will be driven not strictly by scientific studies but largely by your philosophy and how you value different aspects of your life.
Although there is growing evidence of safety regarding testosterone in the setting of prostate cancer, and even possible benefit, the studies are not sufficient to draw firm conclusions.
Given the fact that we are dealing with largely generic products I do not expect any definitive answer to these questions over the next several decades. That does not mean that we are deprived of the information that can help guide a rational decision. We just have to be willing to live with whatever comes next.If a man is experiencing symptoms of low testosterone such as fatigue, poor energy, muscle weakness, diminished sex drive and erections, irritable mood and others then I favor treatment with testosterone.
Given what we now know there is nearly certain benefit in the near term regarding quality of life, and there does not appear to be a risk of accelerating cancer. In fact there are several case studies published in the literature that show men having longer than expected overall survival even in the setting of metastatic prostate cancer to the bone. Men on testosterone therapy have had survival of eight years and beyond in the setting of metastatic bone disease.
Living life at your highest level should always be the priority. None of us are guaranteed the future, but we can be certain of the moment at hand. we make every day it's best by actively rejecting decay and embracing a life of vitality. Ultimately we have more control over how we live, then how long we live.
Full article here: https://pubmed.ncbi.nlm.nih.gov/37326322/
What does it mean when you have "castration resistant" prostate cancer?
In the standard of care conventional treatment pathway castration resistance refers to prostate cancer that has progressed despite maximum testosterone blocking therapy.
At this point cancer is considered incurable, and ultimately fatal. There is no treatment currently available that can reverse the progression of cancer when it is at this point. These sobering facts need to be weighed carefully as a man contemplates how to manage this chapter of life.
More than ever my focus turns toward preserved quality and vitality since the days are numbered regardless of the path you choose. Although the cancer is fatal at this point lifespan is still measured in months to years.
Review of recent study of Pluvicto
The FDA has approved drug for castration resistant prostate cancer. In the study published in the New England Journal of Medicine from 2021 it demonstrated superior progression free survival, and overall survival compared to conventional testosterone blocking therapies.
The progression free interval for Pluvicto was 8.7 months versus 3.4 months for androgen deprivation treatment. The overall survival was 15.3 months versus 11.3 months. Grade 3 or higher adverse effects with Pluvicto was 52.7%.
Intellectual Medicine interpretation
The treatment involves an infusion of a radioactive drug every six weeks. The drug is designed to be attracted to prostate-specific membrane antigen (PSMA) thereby concentrating its effect on the prostate cancer tumors. For one week after administration a patient is felt to be a risk to others around him therefore he must limit contact since he is radioactive.
Although the authors describe the side effects as having no adverse effect on quality of life, a grade 3 adverse event is one which substantially interferes with activities of daily living. Grade 4 is an adverse event that is potentially life-threatening.
In summary with significant time spent in treatment, and significant consequences from treatment the net gain in overall survival is four months. Disease will progress, and death will eventually occur despite treatment. This type of marginal gain at significant expense and risk is frequently over-promoted in conventional medicine.
The comparisons are between 2 harmful therapies. There is no comparison between the drug, and alternative protocols.
The decision whether or not to implement Pluvicto or other conventional drug treatment at this point is very much driven by your personal philosophy. How important are those four months? Are you willing to suffer to achieve them? Bear in mind that you are in the process of navigating the final chapter of your life and the terminal event cannot be avoided.
Given its significant imposition on quality of life, and marginal life extension, Pluvicto and other conventional therapies are not pathways that I recommend. The spirit of maintaining vitality supersedes grasping at a few extra months.
Lutetium-177–PSMA-617 for Metastatic Castration-Resistant Prostate Cancer: https://pubmed.ncbi.nlm.nih.gov/34161051/
Which MRI should be used for the prostate?
MRI equipment is rated based upon the magnetic field strength which is recorded in "Tesla" units.
There are two major types of MRIs available in the United States, a 3.0 and a 1.5 Tesla unit.
The 3.0 unit has a more powerful magnet. The test can generally be done more quickly, and does not require a rectal coil which is used in some of the 1.5 unit MRI machines in order to enhance image quality.
If cost is not a factor I recommend the 3.0 T MRI without rectal coil. It is the most comfortable, fastest, and highest-quality imaging.
However the 1.5 Tesla is quite excellent and provides imaging that is sufficient for analyzing treatment pathways in my protocol.
If 1.5 Tesla equipment is chosen, the rectal coil is helpful to enhance the image.
In either case I recommend doing the image without intravenous contrast. The contrast commonly used is gadolinium which is a heavy-metal that accumulates in the body, including in the brain.
The consequences of gadolinium deposition throughout the body are not known, but I can't think of anything good that would likely come from that. In addition there is a risk of reaction to the dye as well as stress on the kidney.
Cost is a factor. If you're paying out-of-pocket be sure to shop around. Price differences can be dramatic. Generally speaking a 1.5 Tesla machine will be less expensive than the 3.0 equipment.
By skipping the intravenous contrast not only will the study be more safe, but it should be less expensive as well. Be assertive when scheduling your MRI. You cannot be forced to use IV contrast, simply tell them you are concerned about adverse reactions. Whenever I order the study I explicitly annotated it as "without contrast."
What if your insurance "requires" a biopsy prior to the MRI?
This is patient abuse. There is no biological, pathological, or logical reason to compel a man to get a biopsy before the MRI. Reject this, appeal the insurance company, get your doctor to advocate on your behalf, and ultimately if needed pay out-of-pocket.
Be prepared for your MRI to have abnormalities within it. It is hard for me to recall any prostate MRI done in a man over 50 that was stone cold normal, or a "PI-RADS = 1."
For reasons most of you are already aware I never recommend a biopsy. The MRI is simply informative and it will help create a baseline for future comparison. If you get a report that appears ominous you still have time to pause, reflect and do your research.
Do not do anything irreversible until you have had time to acquire multiple sources of information.
Join the Facebook Community
Our private Facebook group is where all the conversations are happening. Members of the group get early access and more chances to talk one-on-one with Dr. Petteruti.
Please remember, when requesting to join, share your email address in the questions. We need it in order to ensure your data matches.
Join the Group
