
What Happens During a Prostate Biopsy? Risks, Recovery, and What to Expect
May 26, 2026Prostate biopsy has become one of the most commonly performed procedures in modern urology. Roughly 1 million prostate biopsies are performed every year in the United States. For many men, the path feels automatic. PSA rises, concern follows, and biopsy is presented as the obvious next step.
What concerns me is how rarely men are encouraged to stop and ask a much more important question before agreeing to the procedure. Do I actually need this biopsy right now?
A prostate biopsy is not a neutral event. It is not merely a routine diagnostic step without consequences. It is an invasive procedure with real physical risks, psychological consequences, and significant limitations in what it can tell us.
Many men are told the biopsy is simple, routine, and necessary. Sometimes that is true. Sometimes it is not. Understanding what happens during a prostate biopsy is important. Understanding whether you need one in the first place may be even more important.
What is a Prostate Biopsy and How is it Done?
A prostate biopsy is considered the conventional gold standard for diagnosing prostate cancer, but men need to understand exactly what that procedure involves before agreeing to it.
A biopsy is not a simple blood test or harmless screening tool. It is an invasive procedure in which tissue samples are physically removed from the prostate using a large core needle and examined under a microscope for abnormal or cancerous cells. The goal is to determine whether cancer cells are present and, if found, how aggressive those cells appear based on pathology grading.
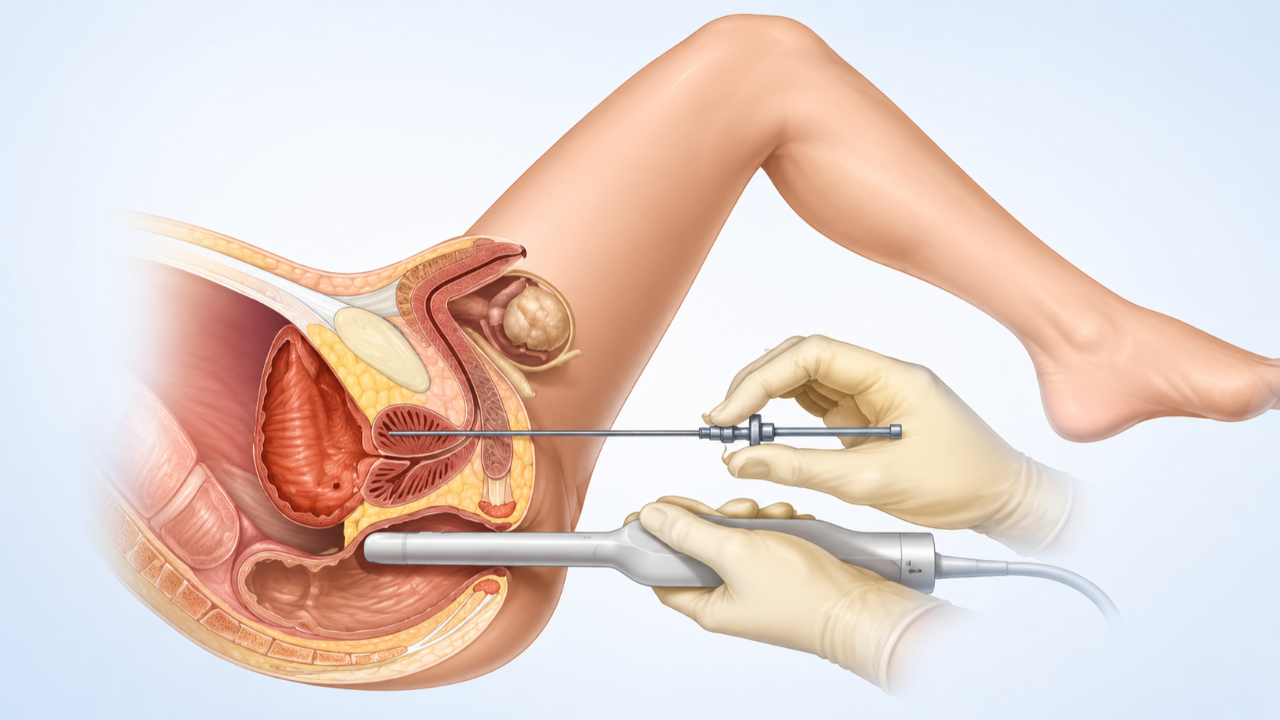
The most common method is a transrectal ultrasound-guided biopsy, often called a TRUS biopsy. During this procedure, an ultrasound probe is inserted into the rectum to visualize the prostate while an 18-gauge needle is repeatedly fired through the rectal wall and into the prostate gland to collect tissue samples. Most men undergo 10 to 14 needle passes, though some biopsies involve even more.
A large needle is being driven through the protective capsule of the prostate over and over again, piercing the gland multiple times in order to sample small pieces of tissue. The procedure itself usually takes 15 to 30 minutes, but the consequences of that decision deserve much more serious consideration than most men are given.
A newer approach, called transperineal biopsy, accesses the prostate through the skin between the scrotum and rectum rather than through the rectal wall. This approach appears to lower infection risk, but it does not change the bigger issue. A needle is still repeatedly penetrating the prostate capsule to obtain tissue.
This is where men need to think critically about what a biopsy actually tells us and what it does not.
One of the biggest limitations of prostate biopsy is something many men never fully understand before agreeing to it.
A biopsy examines only tiny pieces of tissue taken from a very large gland. Even when 10 to 14 cores are collected, only a small fraction of the prostate is actually sampled. That creates a major limitation from the start. If the needle misses the wrong area, clinically significant disease can be missed entirely. This is why false negatives happen and why so many men end up on the biopsy treadmill, moving from one biopsy to the next because PSA remains elevated or imaging continues to raise concern.
But the deeper problem goes beyond missed cancer.
Even when a biopsy finds abnormal or cancerous cells, that information is often treated as far more definitive than it truly is. A pathology report can assign a Gleason score or Grade Group based on how those cells appear under a microscope, but that is still only a snapshot of a small amount of tissue taken at a single point in time.
And that snapshot cannot reliably tell you how the disease will behave.
This is where I believe prostate cancer care often gets the conversation wrong. Men are frequently told biopsy is necessary to determine how aggressive their cancer is. I disagree with that premise. Aggression is not defined by what a few cells look like under a microscope. Aggression is defined by behavior over time.
Is PSA stable, slowly rising, or rapidly doubling? What does MRI show? Is disease contained within the capsule, or is there evidence it is extending beyond it? Those questions tell us far more about biological behavior than a one-time tissue sample.
There is another critical point many men overlook. The presence of prostate cancer cells does not automatically mean danger.
Autopsy studies have shown for decades that many men, especially as they age, harbor microscopic prostate cancer cells without ever developing symptoms, metastasis, or life-threatening disease. In other words, many men die with prostate cancer, not from it.
Modern medicine has become very good at finding abnormalities. But finding abnormal cells is not the same as proving meaningful risk. Detection alone does not tell us whether immediate treatment is necessary, or whether those cells may remain biologically quiet for years.
This is why biopsy results should always be interpreted with caution and in context. A biopsy can confirm that abnormal cells are present. What it cannot do with certainty is predict the future. That uncertainty deserves far more humility than it is often given when life-changing treatment decisions are being made.
Why Prostate Biopsy Deserves More Scrutiny
A common questions I hear from men is simple: Should I get a prostate biopsy? For many men, the recommendation feels automatic. PSA rises, concern escalates, and biopsy quickly becomes the next step. The process often moves so fast that very little time is spent asking whether the biopsy is truly necessary at that moment. The underlying assumption is that more information is always better and that identifying cancer as early as possible must improve outcomes. On the surface, that sounds logical. The problem is that prostate cancer has never been that simple.
I believe prostate biopsy deserves far more scrutiny than it typically receives. It is often presented as a routine diagnostic step, almost as though it carries little downside. That framing minimizes the reality of what biopsy is and what follows after it. A biopsy is not a trivial event. It is an invasive procedure with real physical risks, meaningful psychological consequences, and significant limitations in what it can tell us. More importantly, the consequences of biopsy often extend well beyond the procedure itself.
In many ways, the most significant consequence begins not during the biopsy, but after it, when the pathology report returns with a single word that changes everything: cancer.
That word carries enormous weight. It immediately changes the emotional landscape for the patient and his family. Even when the findings suggest low-grade disease. Even when the lesion appears small. Even when the biology suggests the abnormal cells may remain dormant for years or decades. Once cancer enters the conversation, fear usually follows close behind.
This is where decision-making often begins to shift in the wrong direction. Men who felt calm and rational days earlier suddenly feel urgency. Spouses feel urgency. Families feel urgency. The pressure to act intensifies quickly. The conversation often moves away from thoughtful analysis and toward immediate intervention. Something must be done. Something must happen now. That emotional momentum can become far more powerful than the actual biology of the disease.
The real question is not whether a biopsy can detect cancer. Of course it can. The more important question is whether finding that cancer meaningfully improves the long-term outcome for the patient. Does it improve survival? Does it improve quality of life? Does it lead to better decision-making, or does it simply push men more quickly into a cycle of fear, procedures, and treatments that carry their own significant harms?
That is a much more difficult question, and it deserves far more attention than it typically receives. Before agreeing to a prostate biopsy, every man should pause long enough to ask not only what the biopsy might find, but what that information is likely to change and where that path ultimately leads.
What Recovery Really Looks Like After a Prostate Biopsy
One of the most common things men are told before a prostate biopsy is that recovery is simple. The procedure is often described as routine, minor, and easy to tolerate. For some men, that proves true. They experience mild symptoms that resolve quickly and return to normal within a few days.
But that is not every man’s experience.
For many men, recovery is more uncomfortable and more disruptive than they were led to expect. This is one of the reasons I believe men deserve a far more honest discussion before agreeing to the procedure. Understanding what recovery actually looks like allows men to make better decisions and helps prevent unnecessary anxiety when symptoms develop afterward.
The most common side effect after biopsy is bleeding. Blood in the urine is extremely common during the first several days after the procedure and usually improves with time. Blood in the stool may also occur briefly, particularly after a transrectal biopsy. What many men are least prepared for, however, is blood in the semen. This often persists much longer than expected. In some men it resolves in a few weeks. In others it can persist for six to twelve weeks or longer. While this is usually not dangerous, it can be psychologically unsettling, especially when no one adequately prepared them for it.
Pelvic discomfort and soreness are also common after biopsy. Many men describe rectal tenderness, pelvic aching, or a bruised sensation in the perineal region during the first 24 to 48 hours. The discomfort is often manageable, but it should not be dismissed. Most men improve steadily over several days, though strenuous exercise, heavy lifting, and physically demanding activity are best avoided during early recovery. If pain worsens instead of gradually improving, that deserves prompt medical attention.
Urinary symptoms are also common. Some men experience increased urgency, frequency, burning with urination, or temporary slowing of urinary flow due to irritation and swelling near the urethra. These symptoms usually improve within several days to a week. Occasionally, swelling becomes significant enough to interfere with bladder emptying and cause urinary retention. That is not something to ignore or manage at home.
Even with antibiotic prophylaxis, infection remains one of the most clinically significant risks associated with prostate biopsy. This is especially true with transrectal biopsy, where bacteria from the rectum can be introduced into the urinary tract and bloodstream during the procedure. Studies have shown rising rates of infectious complications over time, driven in part by increasing antibiotic resistance. Reported infection rates after biopsy range from 1% to 6%, with some studies showing hospitalization rates for infectious complications as high as 6.3%. Severe infections, including sepsis, remain a serious concern, with one study reporting sepsis in 2.2% of patients following biopsy. These risks matter because, while relatively uncommon, they represent potentially serious complications tied to a diagnostic procedure many men assume is routine and low risk.
Fever, chills, worsening pelvic pain, or feeling significantly unwell in the days after biopsy should never be dismissed. These symptoms require immediate medical attention. This concern is one reason more physicians are moving toward transperineal biopsy techniques, which appear to reduce infection risk compared with traditional transrectal biopsy. Transperineal vs Transrectal Prostate Biopsy Study Even so, no biopsy is without risk.
Most men recover without major complications. But recovery is not always as minor or insignificant as it is often presented. That is precisely why every man should understand both the short-term side effects and the broader implications before agreeing to move forward.
What a Prostate Biopsy Can Tell You—and What It Cannot
A negative biopsy result, meaning no cancer found in the sampled tissue, offers reassurance but not certainty. The needle samples only a fraction of the prostate's total volume. Cancer can be present in regions that were not sampled, which is why physicians sometimes recommend repeat biopsies when clinical suspicion remains elevated despite a clear result. A positive result will include a Gleason score, a grading system that describes how aggressive the cancer cells appear. Lower scores suggest a slower-growing disease. Higher scores indicate cells with more significant alterations.
What a biopsy cannot tell you is whether the cancer it finds, if any, will ever cause you harm. That distinction sits at the center of one of the most important conversations in modern prostate cancer medicine.
How to Approach the Conversation with Your Doctor
Before agreeing to a prostate biopsy, I believe every man should slow down and ask better questions. Too often, the conversation moves far too quickly. PSA rises, concern escalates, and biopsy is presented as the obvious next step. The momentum of the medical system naturally pushes toward action. Something abnormal is found, so something must be done. That mindset is understandable, but it does not always lead to the best decisions.
The first thing a man needs to understand is the context of his PSA. How elevated is it really? Is it mildly elevated, moderately elevated, or rapidly rising? Has it been stable for years with small fluctuations, or is there a clear upward trend? These distinctions matter. A single PSA value rarely tells the whole story. PSA must be interpreted in context, not in isolation.
From there, the conversation should shift toward gathering better information before moving toward invasive testing. Has an MRI been performed? Should imaging be done first? Are there additional factors such as prostate size, inflammation, recent illness, infection, or other benign causes that could explain the PSA rise? These questions deserve careful consideration because they often change the overall picture.
Perhaps the most important question, however, is one that many men never think to ask. If this biopsy is positive, what exactly changes? What is the likely next step? Does the result lead to meaningful action that improves long-term outcomes, or does it simply move you further down a pathway of escalating intervention? That question deserves honest discussion because it forces both the physician and the patient to think beyond the immediate procedure and focus on the larger strategy.
Men should also ask whether time is truly working against them. Is there a meaningful clinical downside to slowing down, repeating PSA testing, obtaining imaging, or monitoring the situation more closely before proceeding? In many cases, taking more time does not worsen outcomes. It simply allows for better decisions made with greater clarity and less fear.
A thoughtful physician welcomes these questions. In fact, a good physician appreciates a patient who wants to understand the reasoning behind a recommendation. If your doctor cannot clearly explain why a biopsy is necessary right now, rather than after further evaluation, that should give you pause.
This is your body. This is your health. And these decisions carry real consequences. You should never feel rushed into an invasive procedure simply because fear has entered the conversation. The best decisions are rarely made under pressure. They are made with clarity, logic, and a full understanding of both the short-term and long-term consequences.
Common Questions About Prostate Biopsy
Men considering a prostate biopsy often ask the same questions, and understandably so. The decision carries more weight than many initially realize.
One of the most common questions is whether the procedure is painful. Most men describe the biopsy itself as uncomfortable rather than severely painful, particularly when local anesthesia is used. The procedure usually takes only 15 to 30 minutes, and most men are in and out of the office within about an hour. In many cases, the recovery is more disruptive than the biopsy itself.
Another common question is when symptoms after biopsy become concerning. Mild bleeding, soreness, and urinary irritation are common during recovery. What should never be ignored, however, is fever, chills, worsening pain, inability to urinate, or feeling significantly unwell. Those symptoms require prompt medical attention.
Many men also ask whether waiting before agreeing to biopsy is reasonable. In many cases, the answer is yes. That decision depends on the PSA trend, MRI findings, overall risk factors, and the broader clinical picture. Not every elevated PSA requires immediate biopsy. Often, slowing down allows for better information and better decisions.
A negative biopsy raises another common question: does this mean everything is clear? Not necessarily. A negative result means no cancer was found in the tissue that was sampled. It does not guarantee cancer is absent, since biopsy evaluates only a small fraction of the prostate. This is one reason context and long-term monitoring still matter.
A prostate biopsy is not a minor decision. It carries real risks, real side effects, and real limitations in what it can tell you. While biopsy can detect cancer, the more meaningful question is whether the information gained will truly improve your long-term outcome or lead to better decisions.
At Intellectual Medicine, we believe longevity and quality of life should never be treated as opposing goals. Preserving vitality, strength, independence, and sexual health matters. No man should feel pressured into an invasive procedure driven by fear, urgency, or incomplete information.
The best decisions in medicine are made through clear thinking, careful evaluation, and honest discussion of both risks and benefits. Sometimes the smartest decision is not what you choose to do next. Sometimes it is what you choose not to do.
If you want a deeper understanding of prostate biopsy, PSA interpretation, and how to think more clearly about prostate cancer decisions, watch Dr. Petteruti’s full podcast - Think Twice Before a Prostate Biopsy, The Evidence You Need to Hear
About Dr. Stephen Petteruti
Dr. Stephen Petteruti is a physician focused on men’s health, hormone optimization, longevity, and prostate cancer care. His approach challenges conventional thinking by focusing on root causes, metabolic health, and long-term vitality. His goal is not simply helping patients live longer, but helping them preserve strength, energy, resilience, and quality of life as they age.
Learn more at https://www.drstephenpetteruti.com
References
- Bhanji Y, Allaway MJ, Gorin MA. Recent Advances and Current Role of Transperineal Prostate Biopsy. Urol Clin North Am. 2021;48(1):25-33. doi:10.1016/j.ucl.2020.09.010
- Hu JC, Assel M, Allaf ME, et al. Transperineal vs Transrectal Prostate Biopsy—The PREVENT Randomized Clinical Trial. JAMA Oncol. 2024;10(11):1590–1593. doi:10.1001/jamaoncol.2024.4000
- Huang S, Reeves F, Preece J, Satasivam P, Royce P, Grummet JP. Significant impact of transperineal template biopsy of the prostate at a single tertiary institution. Urol Ann. 2015;7(4):428-432. doi:10.4103/0974-7796.152052
- Jahn JL, Giovannucci EL, Stampfer MJ. The high prevalence of undiagnosed prostate cancer at autopsy: implications for epidemiology and treatment of prostate cancer in the Prostate-specific Antigen-era. Int J Cancer. 2015;137(12):2795-2802. doi:10.1002/ijc.29408
- Rudzinski JK, Kawakami J. Incidence of infectious complications following transrectal ultrasound-guided prostate biopsy in Calgary, Alberta, Canada: A retrospective population-based analysis. Can Urol Assoc J. 2014;8(5-6):E301-E305. doi:10.5489/cuaj.1751
- Serefoglu EC, Altinova S, Ugras NS, Akincioglu E, Asil E, Balbay MD. How reliable is 12-core prostate biopsy procedure in the detection of prostate cancer?. Can Urol Assoc J. 2013;7(5-6):E293-E298. doi:10.5489/cuaj.11224
- Wu YP, Li XD, Ke ZB, et al. Risk factors for infectious complications following transrectal ultrasound-guided prostate biopsy. Infect Drug Resist. 2018;11:1491-1497. Published 2018 Sep 17. doi:10.2147/IDR.S171162
Ready to take the next step? Schedule your one-on-one consultation with Dr. Stephen Petteruti
Get exclusive insights every month
We hate SPAM. We will never sell your information, for any reason.
Author
